No-Code vs. Low-Code vs. AI-Generated Code for Healthcare Apps: Decision Framework for Founders

You have the app idea, maybe a pitch deck. And 3 ways to build: a no-code platform, a low-code builder, or code an AI writes for you. Every comparison you've read ranks them on speed and cost, as if a patient portal were a food delivery app. The best way to build a healthcare app hangs on one question: what happens once identifiable patient data enters the system?
Healthcare breaches have been the costliest of any industry for 14 years running, averaging $7.42M per incident (IBM 2025). And the wrong build choice usually works fine at launch. The bill arrives later, as a rebuild quote mid-fundraise or an enterprise deal stalled on a security questionnaire.
You'll walk away with 3 tools for the call: a 10-criteria decision matrix, 4 founder scenarios that end in explicit recommendations, and a 5-question self-assessment that maps your answers to a build path.
What's the best way to build a healthcare app: no-code, low-code, or AI-generated code?
Match the approach to the situation: no-code fits non-PHI prototypes only, since most platforms won't sign a BAA. Low-code/AI-assisted platforms fit PHI-handling MVPs through production, with the BAA, audit logging, PHI-safe defaults, and code ownership built in. Custom development fits deeply differentiated products where the code itself is the moat.
Key Takeaways:
- Healthcare flips the build-approach question from savings to downside. Generic comparisons rank speed and cost; healthcare prices the wrong pick in breach costs ($7.42M average) and an OCR penalty ladder that climbs to a $2.19M annual cap.
- The 10-criteria matrix locates your column fast. No-code stops at non-PHI prototypes, low-code/AI-assisted carries PHI work from MVP through production, and custom is reserved for products differentiated at the code level.
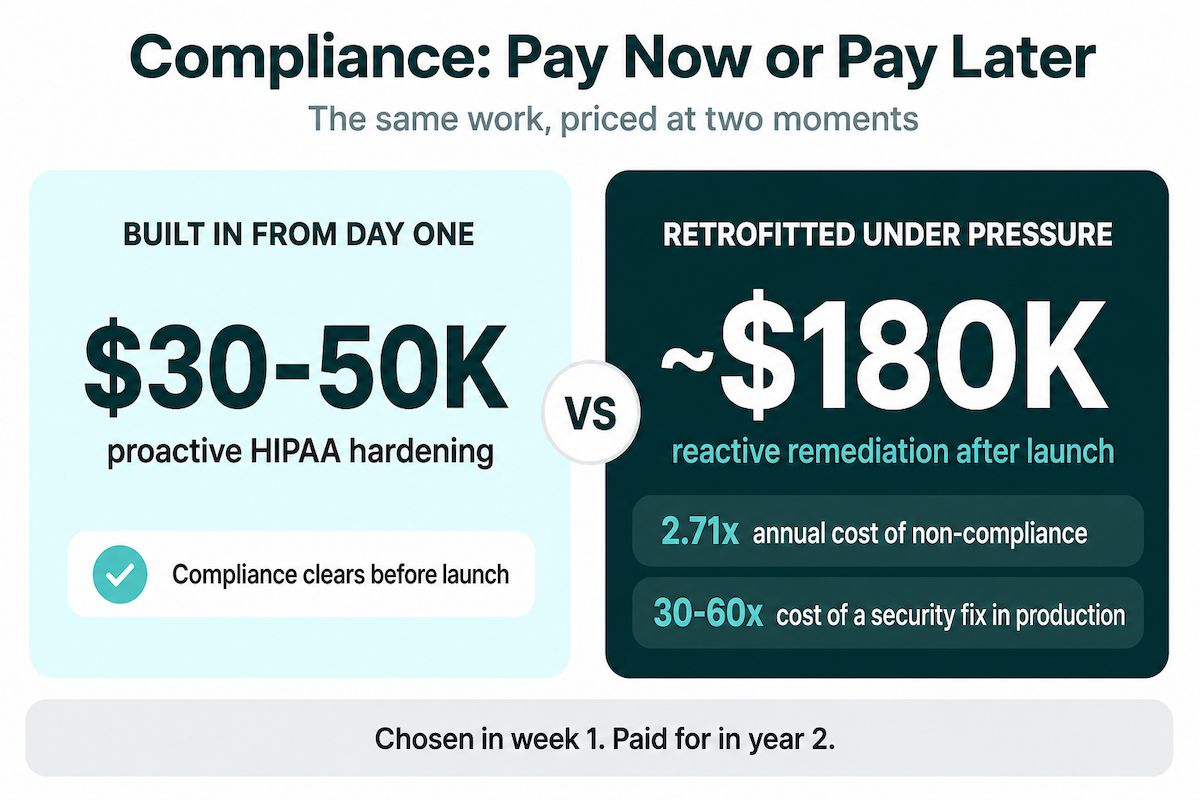
- Choosing wrong bills you later, at documented multiples. Non-compliance runs 2.71x the cost of staying compliant, and reactive HIPAA remediation has run around $180K against $30-50K done up front.
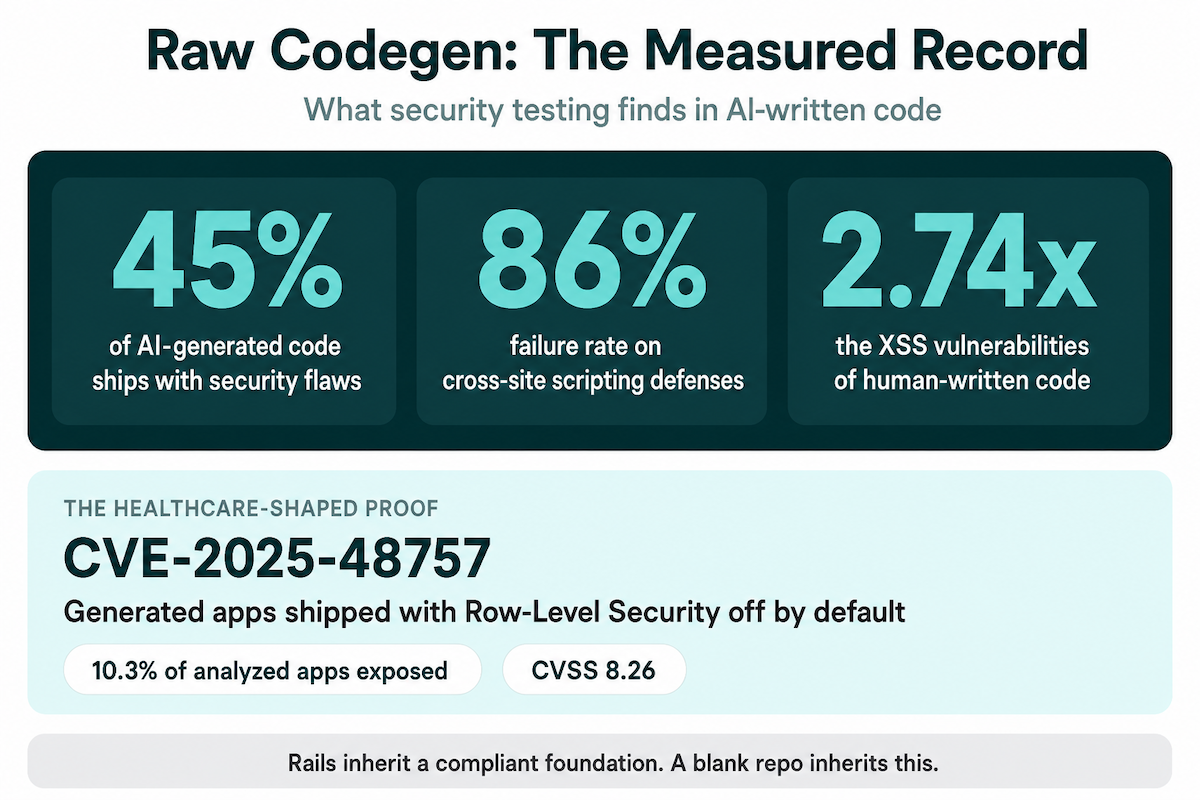
- "AI code" splits into 2 risk categories. Raw codegen carries a measured 45% security-flaw rate and shipped the Lovable CVE; assisted-on-rails generates inside a foundation that was compliant before the first prompt.
- 5 questions make the call. PHI timing, vendor BAAs, EHR deadlines, code ownership needs, and the location of your differentiation route you to a column; honest answers decide it for you.
The three paths
No-code platforms hand you a visual builder on hosted infrastructure, with no access to the code underneath. The trade runs fast in the right direction: a clickable MVP in days, real user feedback before you've hired an engineer. It runs just as fast into a ceiling, because the platform owns the code and, with it, your compliance posture. We covered the trap of no-code in healthcare at length in its own post.
Low-code flips the ratio. The platform ships the compliance-sensitive plumbing pre-built (auth, database, audit-friendly data patterns, hosting) and you put custom logic on top. In healthcare this category has quietly become home to AI-assisted builders, where you describe the app in plain English and generation happens inside that foundation. We keep a running guide to low-code platforms for healthcare.
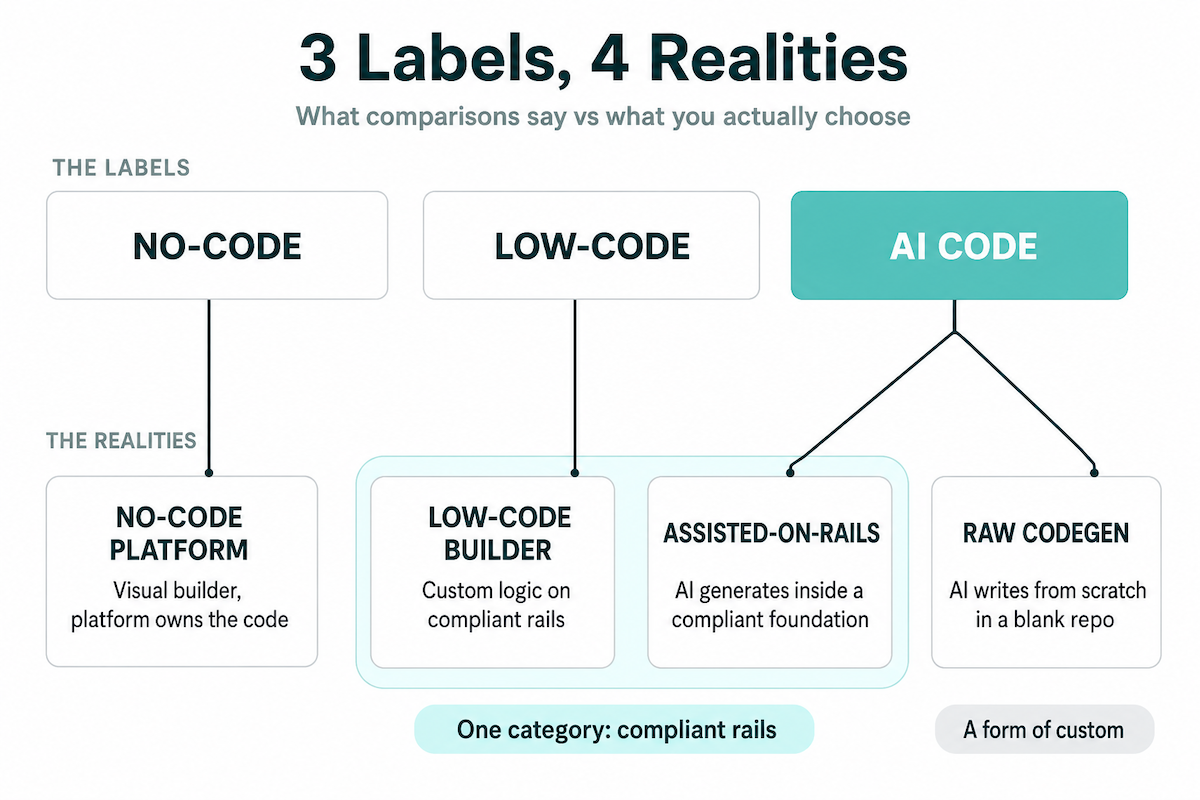
The third label needs splitting before any of this is useful. Most comparisons treat the menu as binary: no-code/low-code. AI code healthcare app building covers 2 different realities.
Assisted-on-Rails
An AI generates your app inside a pre-built compliant foundation, which is really the modern form of the low-code category above.
Raw codegen
An AI writes the whole thing from scratch in a blank repo, which is a way of doing custom development. 3 labels, 4 realities. The decision matrix below keeps those 2 in separate columns, and in healthcare the line between them carries regulatory weight.
Why generic no-code vs low-code advice fails in healthcare
Every generic no-code vs low-code healthcare comparison you'll find ranks the same 4 factors: speed, cost, flexibility, learning curve. Rank them for a project tracker or a booking app and the list works fine. All 4 measure what the right pick saves you. Healthcare swaps the denominator, because here the deciding number is what the wrong pick costs, and those 2 numbers live in different universes.
The constraints generic comparisons never price
Healthcare adds 4 constraints to the pick, and none of them fit in a feature grid:
- Protected health information handling, plus the access controls that keep it defensible in an audit
- A business associate agreement (BAA) with every vendor that touches your data layer, including the platform itself
- Audit logs a regulator can actually reconstruct events from
- EHR integration, if your app ever needs to talk to a hospital
The last one deserves numbers, because founders underprice it on reflex. Read-only FHIR integration starts around $15K; bidirectional runs $150K+. Maintenance adds $3K-15K per interface per year, and hospital approval alone eats 3-6 months before development even starts.
And the platform decides your compliance ceiling before you've built a single workflow. Bubble says it plainly in its own documentation: it doesn't sign BAAs, and apps built on Bubble won't achieve HIPAA compliance. Most no-code healthcare app limitations trace back to exactly this. The ceiling comes from the foundation, and building on top never raises it. We cover the full constraint set in our post on HIPAA compliance in no-code development.
The penalty asymmetry in numbers
Start with the breach itself. IBM's 2025 report puts the average healthcare breach at $7.42M, with 279 days to identify and contain against a 241-day global average. Then the regulator: after the January 28, 2026 inflation adjustment, OCR civil penalties run $145 per violation up to a $2,190,294 annual cap.
And OCR closing its file ends nothing. New York's SHIELD Act treats a HIPAA violation as a SHIELD violation in its own right, so the state attorney general gets a swing too. Class actions pile on: the Change Healthcare breach has already produced an MDL consolidating 70+ suits.
Set all of it against what the shortcut buys you: a few weeks of saved build time. Weeks on one side, 7 figures and most of a year of incident response on the other. That asymmetry flips the generic calculus.
The floor is rising
HHS has proposed a Security Rule overhaul that strips out the "addressable" flexibility the current rule allows. Under the proposal, 4 safeguards become flat requirements:
- encryption at rest and in transit
- MFA
- audit logging
- annual penetration testing
Still a proposal as of mid-2026, to be clear, and the May 2026 finalization window passed without a published rule. But once a final rule lands, the compliance clock runs roughly 240 days. The practical read: pick the approach that already clears the proposed bar, and the rulemaking timeline stops being your problem.
Every criterion in the matrix below traces back to one of these constraints. That's the difference between a healthcare comparison and a generic one wearing scrubs.
The decision matrix: 10 criteria across 3 paths
A healthcare app development approach comparison lives or dies on which criteria get compared. All 10 below are framed through compliance and clinical workflow needs. How to read the columns: the middle one is where purpose-built healthcare builders live, assisted-on-rails included. The right one covers custom in both its forms, hired engineers or raw AI codegen. The left is classic no-code.
"Platform-dependent" in the BAA row is doing heavy lifting. Bubble, the biggest name in that column, doesn't sign one, as its docs told you two sections back. When the platform can't sign, the cell reads "no" for your app, whatever the marketing page implies.
The spread hiding in the EHR row is the table's widest. "Custom-built" means $15K-$150K+ per interface before maintenance; "built-in" means the platform already did that work.
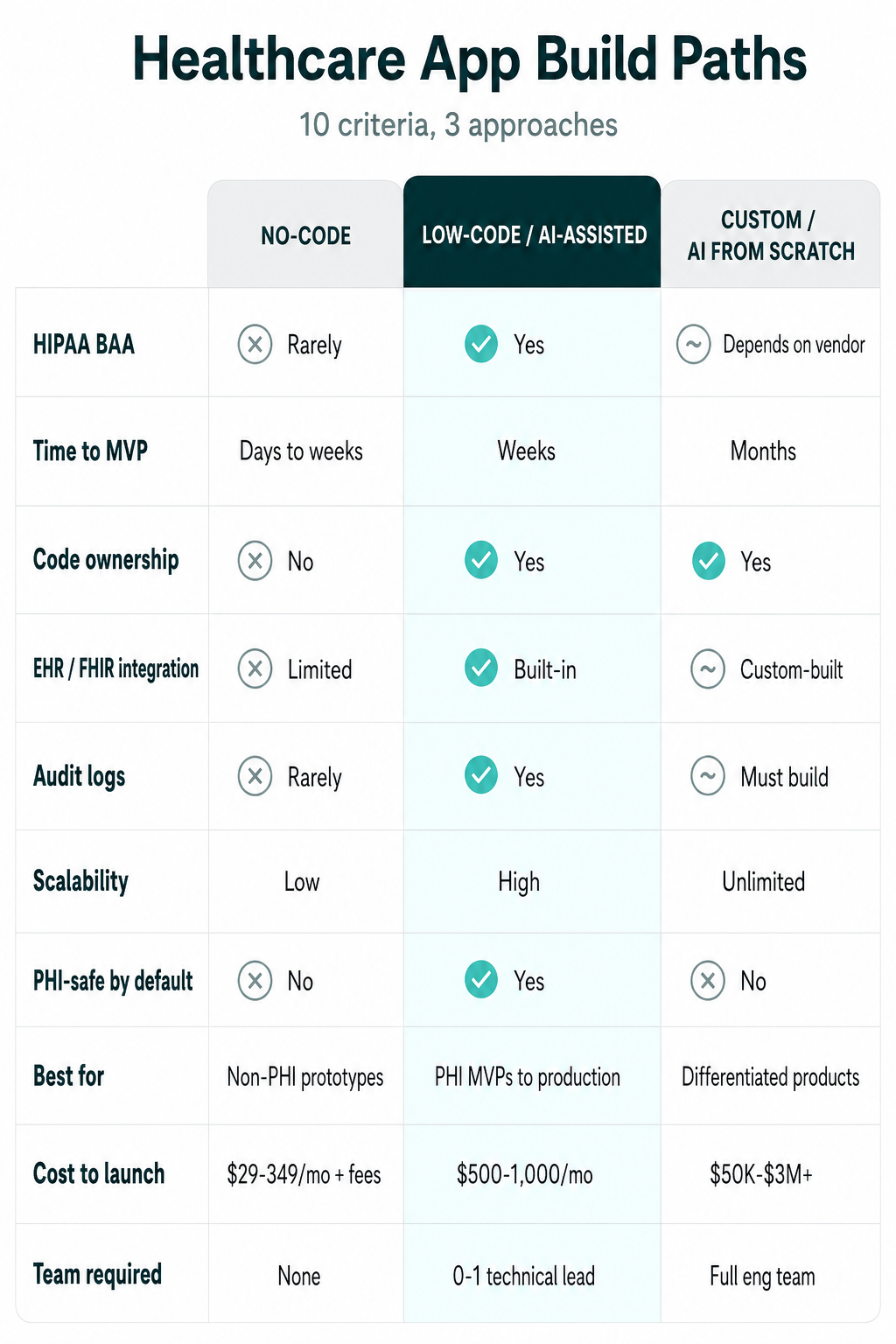
The cost row hedges on purpose. No-code sticker prices start at $29/mo, but production healthcare apps on those platforms commonly run $1,500-3,500/mo all-in once plugins and usage fees stack, and that cheap entry is where vendor lock-in prices your exit. Custom carries its own asterisk: compliance engineering typically adds 15-25% to the build quote.
"Must build" in the audit logs row is also set to get heavier. The proposed Security Rule would make audit logging a flat requirement (still a proposal as of mid-2026), turning that cell from a to-do into a mandate for the custom column.
The matrix tells you what each path gives. The 4 scenarios next tell you which fits your situation.
Which development approach fits your situation: 4 founder scenarios
The matrix ranks attributes. Your situation (PHI timing, team profile, where your differentiation sits) picks which development approach. Healthcare app founders tend to show up in 1 of 4 spots, and each comes with a clear answer. Find yours below; the recommendation at the end of each is meant to be taken literally.
The clinician-founder validating a non-PHI idea
You see the workflow problem every shift and there's no dev team behind you. Nothing identifiable needs to flow yet. Validation is the whole job: mock the intake flow and put a clickable build in front of 20 colleagues. No-code does that job in days for the price of a subscription. The pattern we see most here: a scheduling or referral workflow that spreadsheets are currently duct-taping together.
The boundary that ends the scenario is legal and specific. 45 CFR 160.103 draws that line around anything individually identifiable tied to someone's health condition, or to the care and payment around it. A real patient record entering the build is the tripwire: cross it and you've changed columns, whether or not the app changed.
Recommendation: start on no-code, and write down today which planned feature trips the wire.
The health tech startup with PHI from day one
PHI ships in v1 and speed decides whether there's a v2. For a healthcare startup in this spot, the middle column exists on purpose: compliant infrastructure someone else already built, with your product logic generated on top of it. The whole pitch is subtraction, because the compliance-sensitive plumbing stops being your build while the BAA and the audit trail come with the foundation. That's the column Specode was built for.
Why the neighbors don't fit:
- Custom means months of build plus a hiring plan you haven't funded
- No-code parks you under the BAA ceiling
Recommendation: low-code/AI-assisted. Ship on rails that were compliant before you showed up.
You already vibe-coded a prototype
The prototype did its job: idea validated, maybe even funded. Carrying real patient data is a different job, and the gap between the 2 is bigger than it looks from the demo. We wrote the playbook for HIPAA remediation after a no-code launch; run it before go-live.
Recommendation: remediate first, launch second.
The well-funded team building something deeply differentiated
Your moat is the code itself: a novel clinical algorithm, a device integration, payer-specific workflows no platform ships. A platform can't pre-build what doesn't exist yet, so rails that speed up standard workflows will only constrain yours. Buy rails when your value sits in the workflow. Build when the value is the code, and own everything down to the infrastructure.
Recommendation: custom development on purpose-built infrastructure, compliance engineered in from sprint 1.
The hidden cost of choosing wrong
Healthcare app development failures rarely get public postmortems, and the silence is structural: rebuilds happen quietly, mid-fundraise or under a failed security review. So the decision cost stays invisible right up until it lands on you. Every path in this comparison sells development speed. The wrong one for your situation sells it on credit.
The multipliers and the rebuild bill
The credit comes due at documented multiples. Ponemon's 2017 compliance research puts the annual cost of non-compliance at 2.71x the cost of staying compliant, $14.82M against $5.47M in its large-company sample. Those dollar levels belong to multinationals; the ratio travels down to startups just fine. Defect economics add the second multiplier: a fix shipped in production runs roughly 30x its design-stage cost, up to 60x for security defects, per long-cited NIST and IBM figures. That's technical debt, priced. Compliance debt runs the same curve with a regulator co-signing the invoice.
Founders usually meet these multipliers while relitigating the oldest matchup in the space, no-code vs custom development. Healthcare settles it with invoices instead of opinions. We've seen reactive HIPAA remediation of a vibe-coded app run around $180K in engineering and consulting; the same hardening done up front prices at $30-50K. One shop's numbers, so treat them as directional. A compliant-infrastructure migration at small-company scale runs $50K-250K and takes 2-6 months. Both ranges price the same mistake: software architecture chosen in week 1, paid for in year 2.
The costs that never hit an invoice
Then there's the quieter ledger. An enterprise pilot pauses while your security questionnaire fails. Due diligence stretches to 3x its usual length because the data room can't answer basic PHI questions. Those costs skip the invoice and land in the raise: founders who clear compliance before a priced round spend the round on product, and founders who put it off spend the round on remediation.
The regulatory floor has a case attached. In 2016, OHSU paid OCR $2.7M after ePHI for 3,044 people, diagnoses and Social Security numbers included, sat in Google Drive and Gmail with no BAA in place with the platform vendor. Swap in any modern no-BAA platform and the pattern holds: off-the-shelf convenience with a regulator's price tag.
The team at HIPAA Vault, who fix these projects for a living, put the volume plainly: "Close to 50% of the work we do is fixing broken projects... companies work for a year or two and never launch."
The cheapest path, over any horizon that includes an audit, is the one you don't rebuild. And 1 of the 3 paths carries its own special version of this problem, measured and getting worse.
AI-generated code: speed without guardrails
One more split and the framework closes. Assisted-on-rails constrains generation inside a compliant foundation; you met it in the matrix's middle column. Raw codegen hands a model a blank repo and ships what comes back, whether the prompt ran through Cursor, Lovable, or Replit. The measured record belongs to that second kind.
The gap is mechanical before it's empirical. Models chase code that runs, and compliance sits outside that objective. Veracode's 2025 GenAI Code Security Report tested 100+ LLMs across 80 coding tasks and found security flaws in 45% of the output, a rate that held flat as newer models shipped. The failures concentrate where healthcare hurts: cross-site scripting defenses failed in 86% of relevant tasks. CodeRabbit's December 2025 review of real pull requests puts multipliers on it: 2.74x the XSS vulnerabilities of human-written code, 1.57x the security findings overall.
And generated code has no concept of PHI. CVE-2025-48757 is the healthcare-shaped proof: Lovable-generated apps shipped with Supabase Row-Level Security off by default, leaving 10.3% of analyzed apps open to unauthenticated reads and writes, CVSS 8.26. Every affected app inherited the insecure default the same way. The rest of the PHI risks in AI-generated code story is its own post.
The human factor compounds the machine one. Developers working with AI assistants wrote measurably less secure code while rating it as more secure, per Perry et al.'s user study. Jens Wessling, Veracode's CTO, is blunt about vibe coding: it leaves secure coding decisions to models that "make the wrong choices nearly half the time, and it's not improving."
The framework's last distinction lives inside AI generated code. Healthcare app generation on rails inherits auth, audit logging, and safe data patterns from a foundation that was compliant before the first prompt. Raw codegen inherits an empty repo and the 45% flaw rate. We keep the longer argument in vibe coding in healthcare.
The 5-question self-assessment
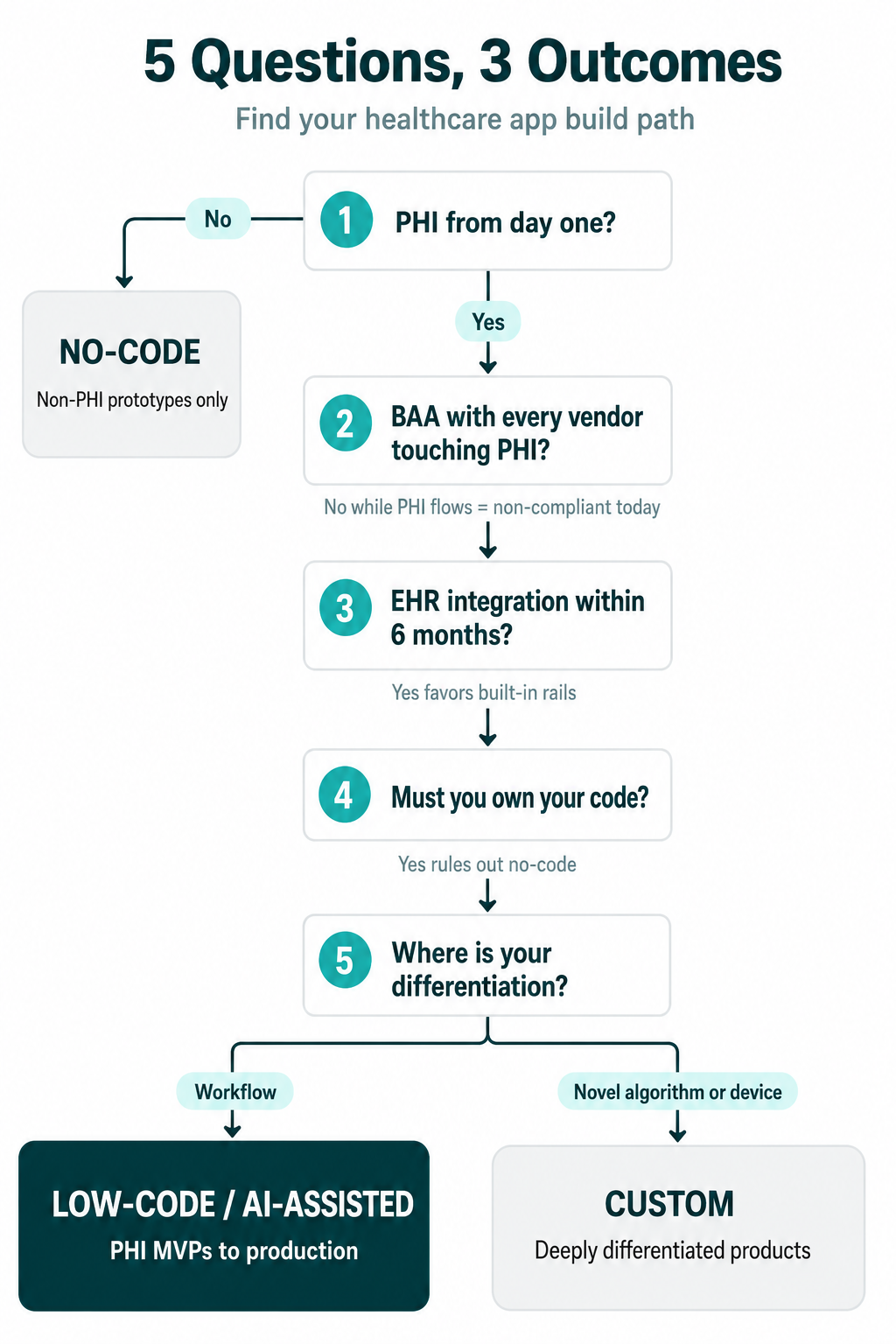
Strip the framework to its studs and 5 questions remain. Honest answers make the medical app development call for you; each maps back to a matrix column and 1 of the 4 scenarios. Build vs buy, asked 5 ways.
- Will your app handle PHI from day one, or is this a non-PHI prototype? A yes moves you to the middle or right column. 45 CFR 160.103 draws the line, and scenario 1's tripwire applies the day real records flow.
- Do you have a BAA in place with every vendor touching your data layer? Any vendor that creates, receives, maintains, or transmits PHI on your behalf has to sign one. A no here while PHI flows means the app is out of compliance today, whatever else it does well.
- Do you need EHR integration within the next 6 months? Hospital approval alone runs 3-6 months before development starts; add weeks for read-only FHIR or months for bidirectional. Built-in beats must-build on a 6-month clock.
- Do you need to own your code for fundraising, enterprise sales, or acquisition readiness? A yes closes the no-code column. Investors and acquirers read code ownership as a line item, and platforms that keep the code keep the upper hand.
- Is your differentiation in the workflow, or in a novel clinical algorithm or device? The answer routes you:
- workflow differentiation to low-code/AI-assisted, where the rails already exist
- a novel core to custom, where scenario 4's logic takes over: own every layer
Score it. Mostly no on PHI and integrations, and a no-code prototype is the honest starting point. PHI plus a speed constraint puts you in the middle column. A novel core sends you to custom. Question 5 is where the low-code vs custom healthcare software decision lands; the other 4 mostly rule columns out.
How Specode fits into this framework
If the scenarios and the 5 questions keep pointing you to the middle column, this is who lives there. We built Specode for the low-code/AI-assisted category specifically, and the fit shows in the matrix's own language, row by row.
The BAA row reads yes because hosting on the Pro plan comes with the BAA included. Code ownership reads yes in writing: TOS Section 8.2 formalizes it: export anytime, deploy anywhere. PHI safety by default means the HIPAA compliance work sits in the foundation, with HIPAA-ready auth, plus the data patterns and workflows built to survive an audit. The EHR row's built-in covers Epic, Cerner, labs, and pharmacy networks. And audit logging comes with its own inspector: a built-in HIPAA Compliance Agent that scans your codebase on demand and splits findings into must-fix and nice-to-fix; fix, re-run, and it re-verifies.
That's the whole pitch, because the framework already made it. Already sitting on a vibe-coded build? Run the Vibe Code Audit and see what the scan finds before a prospect's security review does. And if you're still weighing healthcare app development options, hold each against the matrix. When the middle column keeps winning, start there: weeks to a working build, and a HIPAA compliant app you own outright at the end.
Frequently asked questions
Yes, for non-PHI validation. Budget the migration before PHI enters: compliant migrations run $50K-250K and take 2-6 months at small-company scale.
Raw codegen carries a measured 45% flaw rate, so treat it as unsafe by default. Generation constrained inside compliant rails, with scanning and review, is the workable pattern.
Pre-built compliant infrastructure (auth, audit logging, BAA-covered hosting) with your custom logic on top. The platform carries safeguards you'd otherwise build yourself.
If users are identifiable and health information flows, assume PHI. The line covers anything identifiable tied to a person's condition, or to the care and payment around it.
A non-PHI prototype takes days. A PHI-ready build on a compliant platform lands in weeks, against months for custom.
Platform-dependent. Some lock code in; purpose-built healthcare platforms export full source. Check export rights in the terms before you build anything.






