How to Build a Patient Referral Management System

A referral gets written in the exam room and faxed to a specialist's front desk. Then it goes quiet. The referring physician never learns whether the patient was ever seen. If you're planning to build a patient referral management system, that silence is the gap you're closing. And it repeats at scale: more than a third of US patients are referred to a specialist each year, per Milbank Quarterly's foundational review of US referral patterns.
Maybe you're fixing this inside your own network with an internal tool that stops referral leakage. Maybe you're building a platform product to sell to healthcare providers. The build decisions are the same either way, so this guide serves both.
Ahead: how the closed loop works, the exchange rails from fax to FHIR, the compliance rules with sharper teeth than HIPAA, the legal line on charging for referrals, and what a build honestly costs.
How do you build a patient referral management system?
Design it as a closed loop: create the referral with structured clinical context, transmit it over rails the receiving side actually uses (fax bridge, Direct, HL7, FHIR), track status through a unique referral ID, and close the loop when the consult report returns to the referrer. Before pilot, wire the BAA chain, audit logging, and MFA, and measure against a pre-build baseline of scheduling rates and wait times.
Key Takeaways:
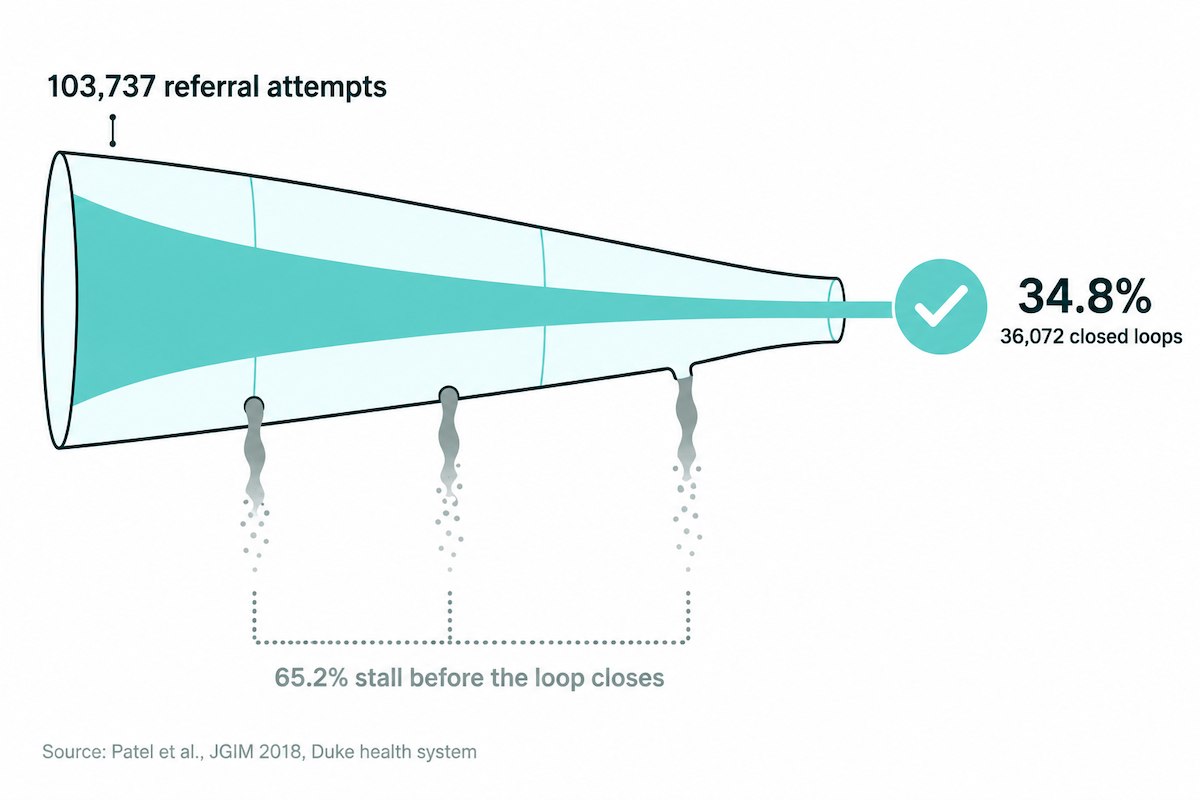
- A patient referral management system exists to close the loop, and most loops stay open today. In Duke's health system data, only 34.8% of 103,737 referral attempts ended with a completed appointment and a report back to the referrer.
- Pick exchange rails before frameworks. With as many as 56% of referrals still traveling by fax, ship fax-in and Direct at launch, and model referral states on the 360X profile so FHIR support arrives later as adapter work.
- HIPAA is the entry ticket; information blocking, 42 CFR Part 2, and the Anti-Kickback Statute carry the sharper penalties. Enforcement is live on all three, from $1M information-blocking CMPs to OIG scrutiny of per-referral pricing.
- The receiving side decides whether your platform lives. The NHS solved adoption with a payment mandate you can't copy, so design for receivers who never signed up: fax bridging and zero-login accept links.
- Cost tracks integration depth. Custom builds run $60K to $450K+ depending on EHR depth; an AI healthcare builder covers web-based referral workflows from $500 a month.
What is a patient referral management system?
A patient referral management system is software that creates, routes, tracks, and closes specialist referrals between a referring provider and a receiving provider. The loop closes when the specialist's consult report returns to the referrer. Everything else in the product (scheduling, messaging, analytics) exists to make that round trip complete reliably.
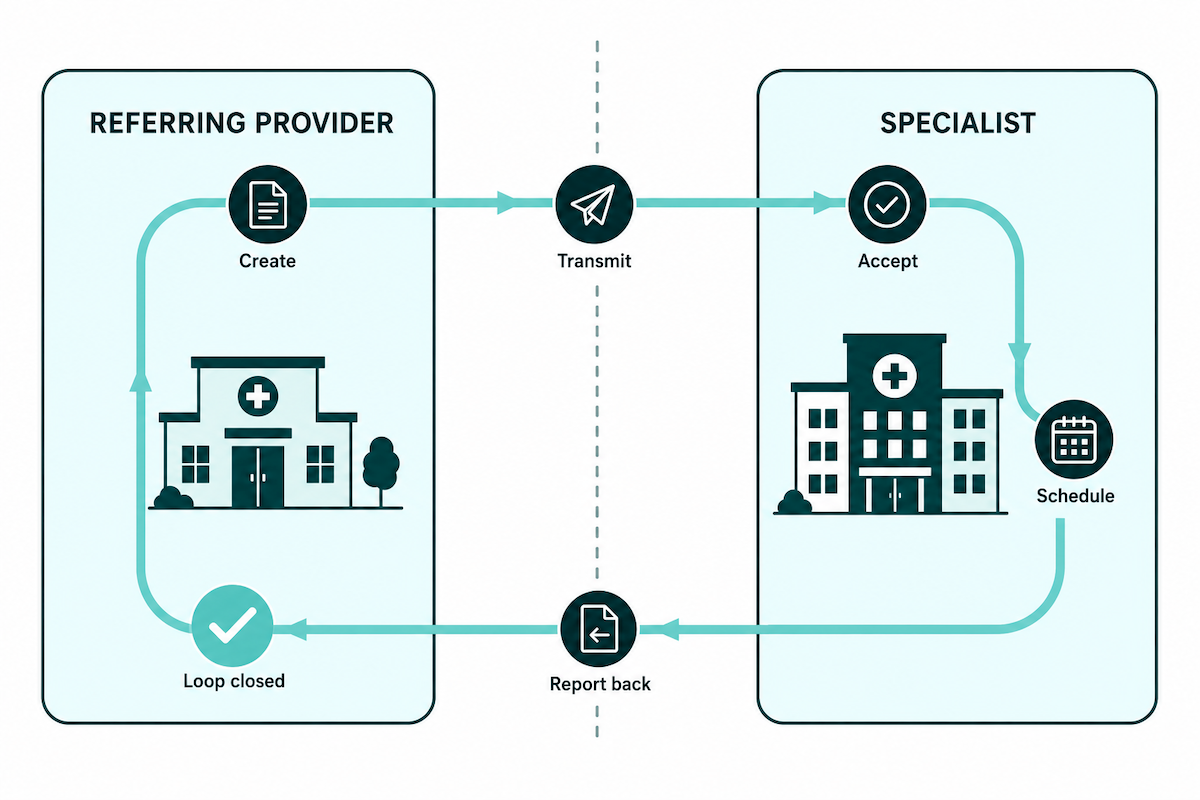
The closed loop is the industry's own frame, and the terminology proves it. CMS tracks closure as quality measure 374, "Closing the Referral Loop: Receipt of Specialist Report," and the referral interoperability profile is literally named 360 Exchange Closed Loop Referral.
The boundary with adjacent tools is state. A scheduling tool books appointments inside one organization; an electronic referral management system tracks a referral's status across two, from the practice that sent it to the practice that received it, until the report comes back.
Why build a patient referral management system: the referral leakage math
You build a referral management system because the default process completes barely a third of the referrals it starts. Inside a clinic that failure feels like small administrative friction: a fax to resend, a voicemail to leave. Added up across a health system, it's a revenue leak you can measure.
The completion number comes from Duke. Patel et al. tracked 103,737 scheduling attempts for specialist referrals across 20 high-volume specialties over a year and counted how many produced both a completed appointment and a specialist report back in the referring physician's hands. The answer: 34.8% (JGIM, 2018). The remaining 65.2% stalled somewhere between the referral order and the consult note.
The revenue side has numbers too. In an October 2018 survey by Fibroblast and Sage Growth Partners, 43% of healthcare executives reported losing 10% or more of annual revenue to referral leakage, the quiet drift of referred patients out of network and into a competitor's schedule. The mechanism is blunt. When a referred patient leaves the network, everything downstream leaves with them:
- imaging
- labs
- procedures
- follow-up visits
Health systems are paying for a fix at matching scale: Grand View Research puts the US patient referral management software market at $7.13B for 2024, compounding at 16.7% a year toward $17.89B by 2030.
Patients feel the same failure as time. The average wait for a new-patient physician appointment hit 31 days in 2025, up 19% since 2022 and 48% since 2004, per AMN Healthcare's survey of 1,391 physician offices across 15 metro markets. The averages hide worse tails: 41.8 days for OB/GYN, 65 days in Boston. A stalled referral stacks its own weeks on top. And under value-based care contracts the leak costs you twice, once in downstream revenue and again in the coordination visibility the contract pays you to maintain.
Whether the thing you ship is an internal tool or a platform product, the value proposition is recovered completions. The referral metrics you'll baseline before writing code (step 2 in the build process below) turn that from pitch into provable number.
Types of patient referral management systems (and which one you're actually building)
"Referral management system" hides 3 different products, and naming yours early prevents a mid-build rework. Before you create a referral management system, settle two axes: direction and topology.
Direction is the simpler call. Inbound tools help the receiving organization capture and triage what arrives; outbound tools help the referring side route patients and track what happens next. The money sits on inbound, which held over 75% of market revenue share in Grand View Research's global analysis.
Topology is where the build diverges, because it decides what you control and which hard problem you inherit:
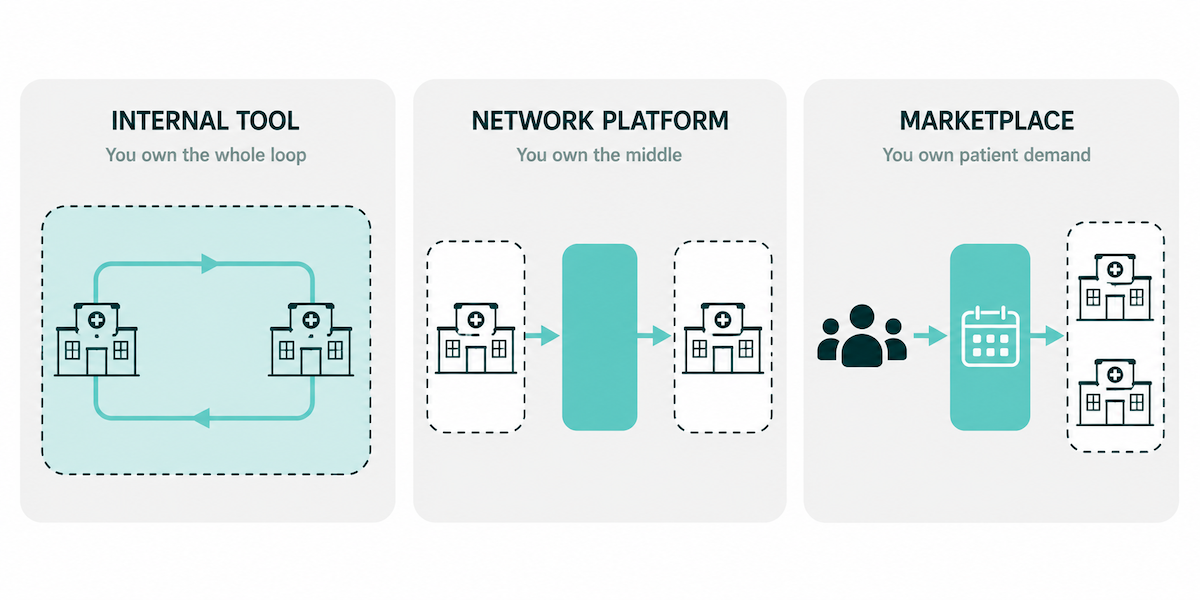
Zocdoc is the marketplace archetype, worth naming because it's the identified requestor behind the OIG advisory opinions in the monetization section. A network platform is a care coordination app at its core: the product is workflows that survive organizational boundaries.
One adjacent modality is worth scoping into any of the three: eConsults, where a specialist answers the clinical question asynchronously and some referrals never need to exist. Across 19 NYC Health + Hospitals specialty clinics, 13% of referral requests were resolved electronically after eConsult rollout (JAMA Network Open). AAMC's Project CORE avoided an estimated 3,600 specialist referrals from 8,000+ eConsults across 5 academic sites in 18 months.
Pick the type first. It sets your integration load and compliance surface, and it decides which revenue models are even legal.
Key features of a patient referral management system, mapped to the referral lifecycle
Most patient referral app development starts from a flat feature checklist. Mapping features to the loop's failure points works better: every stage has a documented break, and a feature earns its place by closing one. The rows below follow the 360X closed-loop flow, plus the analytics layer the profile leaves to you.
Two of those breaks justify specific engineering. Status opacity is the problem referral tracking software gets hired for: one referral ID that survives the round trip across both organizations, with a timeline both sides can see. Stall alerts belong in the same row, because a referral sitting in "sent" for 10 days should page somebody. And the payload gap argues for structured C-CDA attachments, since a specialist working from a 40-page fax scan starts the visit blind.
Schedule-and-outreach is patient engagement work: reminders and self-booking links that pull patients off the phone queue.
The analyze row is revenue infrastructure. Genesis Physicians Group, a 1,500-member Dallas IPA, partnered with Fibroblast in 2019 to run claims-based referral analytics against its value-based contracts. Dashboards that show where referrals leak, and prove network performance to payers, pay for themselves.
MFA and audit logging sit under every stage; the law behind them lands in the compliance section below. And if you want a quick audit frame for an existing process, referrals break at five handoff points (Ideas2IT, directional):
- detection
- scheduling
- outreach
- confirmation
- note return
Run your roadmap against the table. Any feature that can't name its row is decoration.
How to build a patient referral management system in 7 steps
Ask any vendor how to build a referral management system and you'll get a numbered list. The useful version names the decision each step forces, because every step below either shrinks scope or prevents a rebuild.
Step 1: pick your type and loop scope
Carry the typology from above into scope: inbound or outbound, and which handoff points of the referral workflow you own end to end. An internal tool owns the whole loop; a network platform owns the middle. Write it down, because the answer sets your integration list and legal exposure before any wireframe exists.
Step 2: baseline your referral metrics
Instrument the current process before writing code. The Duke study's explanatory factors for open loops are the starting panel:
- scheduling rate
- wait time
- geographic distance
- clinic-level variation
Add the no-shows your front desk already counts. Six months in, these numbers are the only proof that recovered completions are real.
Step 3: choose your integration posture
The fork: EHR-embedded or standalone with bridges. UCSF built its referrals automation as a SMART on FHIR app inside the EHR (Odisho et al., JAMIA Open 2020); embedding buys clinician adoption and costs you a harder build. Standalone with fax-in and Direct bridges ships faster and meets outside counterparties where they are. This one decision moves the budget more than any feature debate, and it shapes the rest of the development process. Referral loops often ship inside a broader virtual-care build; our telehealth app development guide covers that path.
Step 4: design the data model around referral state
State is the product. Model it explicitly:
- a status enum that mirrors the loop (sent, accepted, scheduled, completed, closed)
- a unique referral ID that survives the round trip across both organizations
- a structured clinical payload, C-CDA today, FHIR-shaped for tomorrow
Everything else in the schema hangs off these three.
Step 5: build one thin end-to-end loop
One specialty and one sender-receiver pair. Get the full round trip working, order to returned consult note, before adding any breadth. Closed-loop referrals prove out in depth first; width is a copy-paste problem once the loop holds.
Step 6: wire compliance gates before pilot
Real PHI flows the day your pilot starts, so the gates come first:
- the BAA chain signed with every vendor that touches PHI
- audit logging switched on
- MFA enforced for every role The law behind each gate gets its own section below; here it's a checklist item with a hard deadline.
Step 7: pilot against your baseline, then widen
Run the pilot as quality assurance against real traffic, scored on the step 2 baseline: are more loops closing, and faster? Widen by specialty or site only after the loop holds under load.
On timelines: Specode gets a working prototype in front of you in 20-30 minutes and a production-ready app in 1 to 2 weeks, with Maestro's agents gating each phase on your approval. Traditional timelines, and what they cost, come in the cost section near the end.
What tech stack do you need to build a referral management system?
In healthcare referral management software development, the stack conversation starts with exchange rails. Whatever you build has to speak what the other side already speaks, and most counterparties are further behind than your architecture diagram assumes. The React-versus-Vue debate can wait.
The four exchange rails, from fax to FHIR
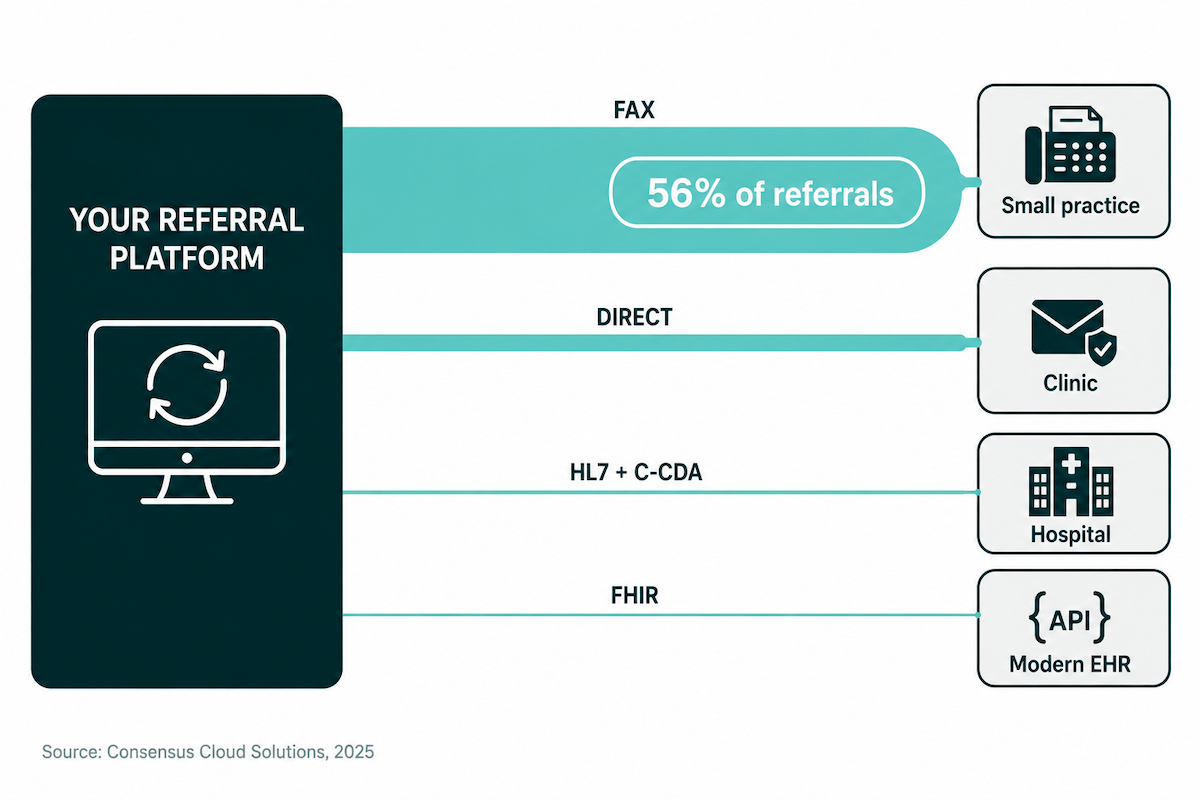
The binding constraint: as many as 56% of referrals are still sent by fax, mostly because of interoperability gaps between systems (Consensus Cloud Solutions, via Medical Economics, November 2025). A referral platform that only speaks modern APIs talks to itself. The receiving side is often a small practice running its day on a practice management system and a fax line.
360X: the closed-loop profile to design against
360X, the closed-loop referral profile from IHE (Rev 1.1, trial implementation), sits on ONC's Interoperability Standards Platform. The specs are freely published and assembled from standards the industry already runs:
- Direct for transport
- HL7 v2 for orders
- C-CDA for clinical content Epic, athenahealth, eClinicalWorks, MEDITECH, NextGen, Netsmart, and Kno2 have all demonstrated 360X exchange (HIMSS interoperability use case).
The FHIR path converges on the same model. HL7's BSeR implementation guide runs referrals on ServiceRequest plus Task, with a referral state machine harmonized with 360X. So model your referral states on 360X now; adding FHIR later becomes adapter work, and your schema survives the transition intact.
One named build for reference: athenahealth's receive-referral implementation packaged the HL7 order and clinical attachments (C-CDA plus PDFs) into XDM for exchange with Epic, Cerner, and any Direct Trust endpoint (practitioner case study).
The pragmatic stack, then: a HIPAA-ready web app and backend, plus an integration layer that ships with fax-in and Direct on day one and adds HL7 and FHIR endpoints where the counterparty can actually receive them.
Compliance and data security requirements: HIPAA is the easy part
When you develop a referral management system, HIPAA is the part your team already knows how to run. The operational core fits in one paragraph. The rules with newer teeth come after it.
HIPAA in one paragraph: the operational core
A BAA chain covering every vendor that touches PHI, hosting included. Minimum necessary applied to referral payloads, so the receiving practice sees the patient data the consult requires and nothing extra. Audit logging on every read and write. Encryption in transit and at rest. Run that list honestly and your referral platform is HIPAA compliant in the sense that matters day to day; the entry ticket is paid. The fines, meanwhile, have moved elsewhere.
Information blocking: enforcement is live
A referral system that hoards or gates electronic health information exchange is the exact conduct information blocking rules target. Think consult notes withheld from a competing network, or referral records that only flow to in-house specialists. HHS-OIG and ASTP issued a joint enforcement alert in September 2025, with Acting Inspector General Juliet Hodgkins promising HHS-OIG will "deploy all available authorities to investigate and hold violators accountable."
The numbers behind the warning: civil monetary penalties run up to $1M per violation for health IT developers, plus health information networks and exchanges. Provider-side disincentives took effect July 31, 2024 and January 1, 2025, with the median hospital disincentive previously calculated at $394,353. And on February 11, 2026, ONC began sending letters of nonconformity to EHR developers, the clearest sign enforcement moved from theory to practice.
42 CFR Part 2: if behavioral health referrals flow through you
Part 2 defines its programs to include providers of SUD diagnosis, treatment, or referral for treatment. Referral is in the definition, so a platform routing behavioral health referrals should assume it's in scope. The compliance deadline passed on February 16, 2026. OCR's Civil Enforcement Program went live three days earlier, and complaints are being accepted. Penalties now match HIPAA's, $141 to $2.1M per violation.
One design consequence worth building early: every consented Part 2 disclosure must travel with the 42 CFR 2.32 redisclosure-prohibition statement, so your payload schema needs a place for it. If you're building in this space, our mental health app development guide covers the wider compliance picture.
The build-stage compliance checklist
Ordered by when each gate has to close:
- Design: flag Part 2 records in the data model; keep payloads minimum-necessary by default.
- Pre-pilot: BAA chain complete, audit logging on, MFA enforced.
- Pre-launch: review any exchange-gating behavior against information blocking rules; run the security review.
One boundary worth naming here: the Anti-Kickback Statute and Stark govern referral arrangements themselves, including how you charge. That's the next section's problem.
Monetization strategies for referral management platforms (without tripping the Anti-Kickback Statute)
The obvious revenue model, charging providers for each referral received, is the legally loaded one. The Anti-Kickback Statute reaches anyone who arranges for federally reimbursable services, and if you build a patient referral app that books specialist visits, that's you.
What OIG blessed at Zocdoc, and what it refused
Zocdoc asked OIG directly and got Advisory Opinion 19-04 (September 2019). The per-booking and per-click fees stood because they were:
- set in advance
- certified at fair market value by independent valuation
- untied to the volume or value of services rendered
- paired with no beneficiary inducements OIG also named what failed: the referral service safe harbor covers only fees based on the cost of operating the service, and Zocdoc's pricing flunked that test.
The framework held under fire: AO 23-04 (July 2023) reaffirmed the position after Zocdoc added spend caps and ranking disclosures, and the Sisselman qui tam was dismissed, affirmed by the Second Circuit in 2025. One catch: advisory opinions bind only their requestor. Replicate the structure, then buy the expertise anyway: independent valuation plus fraud-and-abuse counsel (Frier Levitt, December 2025).
The model menu, ordered by risk
For a referral management platform, the menu sorts itself:
Pick from the top row down. Each step toward per-referral economics buys growth mechanics and a bigger legal bill; Zocdoc's fights above are the price of the middle row.
Where referral management software development goes wrong
A referral system's value depends on the other organization responding, and you don't control them. That dependency, adoption on the receiving side, is where referral management software development actually goes wrong; the code is usually fine.
The cold-start evidence is blunt. When Tasmanian researchers surveyed 204 clinicians on why an e-referral system sat unused, the top barrier was peers not using eReferrals, and 80% were still sending referral letters by fax or post.
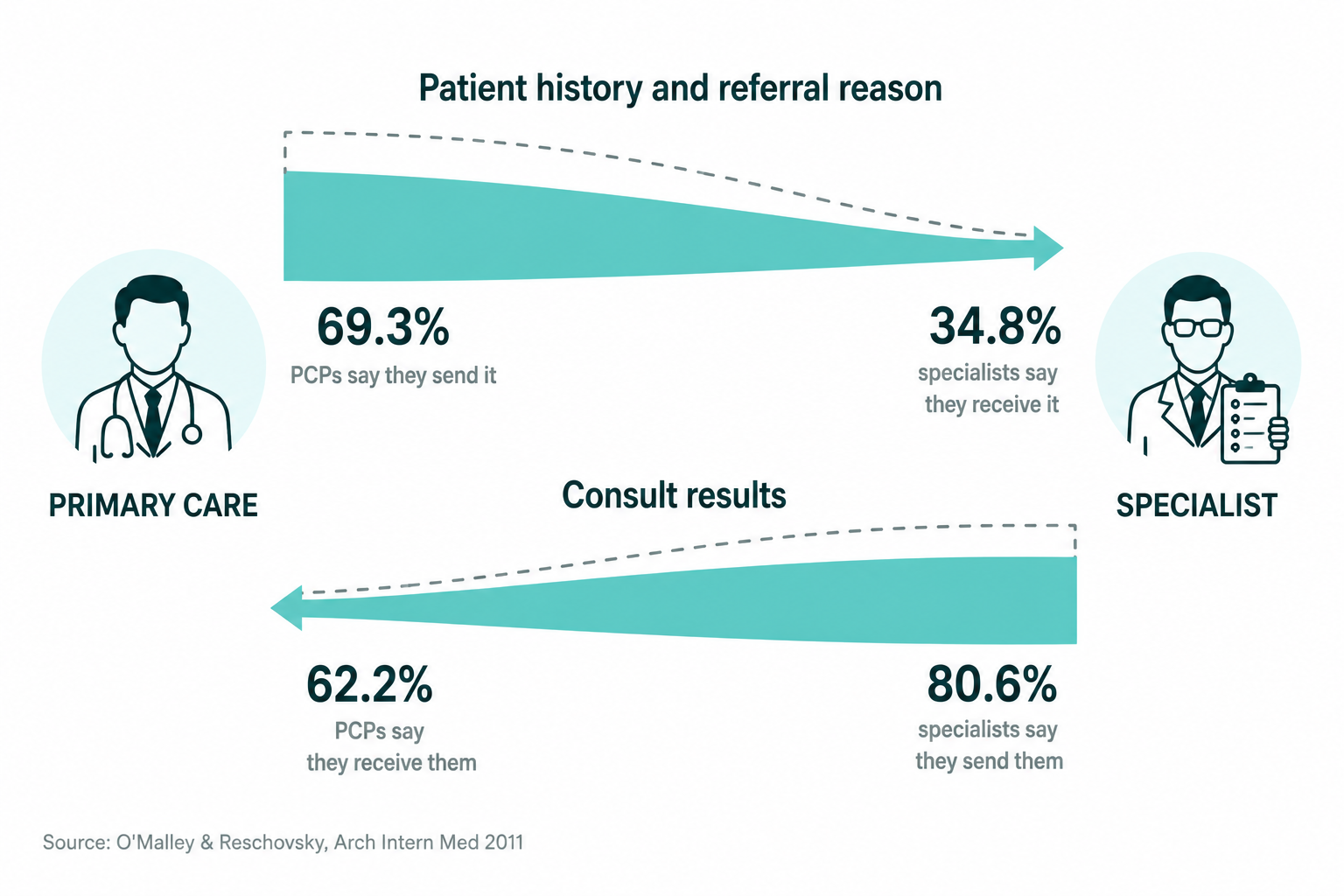
The gap runs in both directions: the primary care physician swears the history went out; the specialist swears it never arrived. The national data backs both. In O'Malley and Reschovsky's national physician survey (Archives of Internal Medicine, 2011), 69.3% of PCPs said they send patient history and referral reason all or most of the time, while 34.8% of specialists said they receive it (coincidentally the same figure as Duke's completion rate above; the two measure different things). Flip the direction and 80.6% of specialists said they send consult results, while 62.2% of PCPs said they receive them.
The one network that beat the adoption problem used a lever you lack. From October 1, 2018, the NHS paid providers only for GP-to-consultant referrals made through its e-Referral Service (Standard Contract SC6.2A). Utilization climbed from roughly 53% to 75% in the run-up year, under a payment mandate, and the mandate is the part a startup can't copy.
So design for receivers who never signed up:
- fax-in and fax-out bridging
- zero-login accept links for recipients
- delivery straight into the EHR in-basket
- value for the sending organization alone, on day one
A tool that earns its keep inside one organization can wait out the network effect. The quieter failure mode, EHR integration cost creep, gets its own numbers next.
How much does patient referral management system development cost?
The straight answer is a range, and integration depth decides where you land inside it. Referral management system development costs scale with how deep you wire into the systems around you; screens are cheap.
Custom build benchmarks and what moves them
On published healthcare app development benchmarks, custom referral builds run $60K to $220K for MVP-to-moderate scope, and $220K to $450K+ once deep EHR integration enters, across 6 to 40 weeks from kickoff to launch.
For a referral product specifically, the moderate tier is where most internal tools land; the advanced tier is network platforms wired into multiple EHRs.
The complexity that moves you between rows is integration depth. Each EHR connection adds its own mapping, certification, and test cycles; read-only access sits at the cheap end, and write-back is where cost climbs. Even a basic integration carries an $8K to $12K floor. Receiver-side UX and compliance hardening stack on top of whatever tier you pick, and your development team will spend more hours on interfaces than on features.
Ongoing reality: plan for 15 to 25% of the initial build annually in maintenance.
The platform path
Specode runs the same build on a HIPAA-ready foundation for $500 a month on Startup or $1,000 a month on Pro, with production deployment and the hosting BAA included on Pro. A working prototype lands in 20-30 minutes, and a production-ready app in 1 to 2 weeks. An optional in-house pen test runs $3,000 if procurement asks.
The honest boundary: the platform path fits web-based referral workflows, and EHR integration stays real, scoped work whichever path you're on. The fax bridge ships fast; the Epic connection is still a project.
How Specode can help
Run the cost drivers from the last section against what Specode ships out of the box. The expensive parts of a referral build are the exact healthcare skills Maestro's agents carry:
- organization topology (single provider through multi-tenant)
- scheduling with provider availability and booking rules
- provider profiles and patient-facing search
- patient intake and onboarding flows
Add real-time secure messaging between the referring and receiving sides, plus SMS outreach through the Twilio skill, and the feature table above starts filling in from prompts.
The HIPAA Compliance Agent covers the compliance checklist from earlier across 11 scan categories, RBAC, audit logging, PHI exposure, API security, and third-party BAA classification among them, with findings split into Must-Fix and Nice-to-Fix. A pre-go-live security review by the Specode team backs the scan before anything touches production.
Code ownership is contractual: you own 100% of the code. Export anytime, deploy anywhere, and if you ever leave, the code transfers to your repo on request.
The honest boundary from the cost section stands: Specode fits web-based referral workflows, and EHR integrations are supported as scoped, real work. Everything else in this guide, the loop, the rails, the compliance gates, the state model, is buildable in weeks. You now know how to create a referral management system; Specode, built by a team with 12 years of experience in health tech, is the fastest place to prove it. Describe your referral loop in plain English and watch the first working version land in about 30 minutes.
Frequently asked questions
Closed-loop software that creates, routes, tracks, and closes specialist referrals across two organizations; the loop closes when the consult report returns to the referrer.
Lifecycle coverage: intake and routing, secure transmission, triage, scheduling with patient outreach, unique-ID status tracking, consult-note return, and analytics.
HIPAA with a complete BAA chain, information blocking rules, 42 CFR Part 2 for SUD referrals, and Anti-Kickback constraints on how you charge.
Roughly $60K to $450K+ custom, driven by EHR integration depth; platform-based builds start around $500 a month.
6 to 40 weeks for custom builds depending on tier; weeks on an AI healthcare builder, with integrations as the long pole.






