Your Health App Is About to go Live, but Is It HIPAA-Compliant?

You built fast. Bubble, Lovable, or another generalist no-code platform, and in a few weeks you had a working app. Now you're about to put real patients into it, which means real PHI, which means exposure you didn't have a week ago. This is your HIPAA remediation healthcare app playbook, written for the founder who shipped first and is reading the fine print second.
It works. Whether it's legal to run on patient data is a separate question, and OCR has been answering it with money. Deer Oaks, a behavioral health provider, paid $225,000 after a coding error in a pilot portal left patient summaries publicly accessible and indexed by search engines. It's the kind of mistake a fast build makes on its own.
The numbers scale from there. In 2026, HIPAA violation penalties run up to $73,011 per violation, with annual caps in the millions. Each violation counts on its own, so one breach involving many records adds up fast. OCR already fines the basics:
- no risk analysis,
- no encryption,
- unsigned BAAs.
The proposed 2026 HIPAA Security Rule would make encryption and MFA mandatory, though it has stalled. The floor is already here.
Timing is the one thing on your side. Retrofitting compliance after launch runs about 3 to 5 times what building it in costs. So run the audit now, then decide what you can patch and what needs to move.
How do you make a no-code health app HIPAA compliant after launch?
Run a six-area audit first: BAAs, encryption at rest, encryption in transit, audit logs, access controls, and breach readiness, then fix what's contractable in about 30 days. For the rest, ask whether the layer holding PHI can get a BAA and enforce access controls, logging, and encryption. If it can't, migrate that layer with a parallel build and incremental cutover before PHI sprawls, since retrofitting after launch runs 3 to 5 times the cost of building it in.
Key Takeaways:
- Live and compliant are two different bars, and the gap gets costly fast. OCR fines the basics, missing risk analysis, encryption, and BAAs, up to $73,011 per violation, and retrofitting after launch runs 3 to 5 times the cost of building it in.
- You can audit your compliance debt today. Check six areas: BAA status, encryption at rest, encryption in transit, audit logs, access controls, and breach-notification readiness. Each is a yes/no you can answer right now.
- The gap usually lives in your builder layer. Bubble and Lovable rarely offer a BAA there, and even on a contractable backend, coverage stops the moment PHI flows into an integration, AI field, log, or export.
- Every tool that touches PHI needs a BAA. One unsigned vendor breaks the whole chain. GoodRx and BetterHelp paid millions to the FTC over tracking pixels, and neither was even a covered entity.
- Most gaps fix in 30 days; the rest mean migrating. If the PHI layer can't get a BAA or enforce controls natively, move it with a parallel build and incremental cutover, ideally before PHI sprawls into logs and backups.
The compliance debt audit: your no-code health app compliance checklist
Compliance debt is the debt you took on to ship fast. Like any debt, it accrues quietly and comes due at the worst time, which here is the day real PHI goes live. It's countable, though. And unlike most technical debt, you can audit this one in an afternoon. This no-code health app compliance checklist is a set of yes/no questions you can answer today, before patients pile in.
The six checks to run today
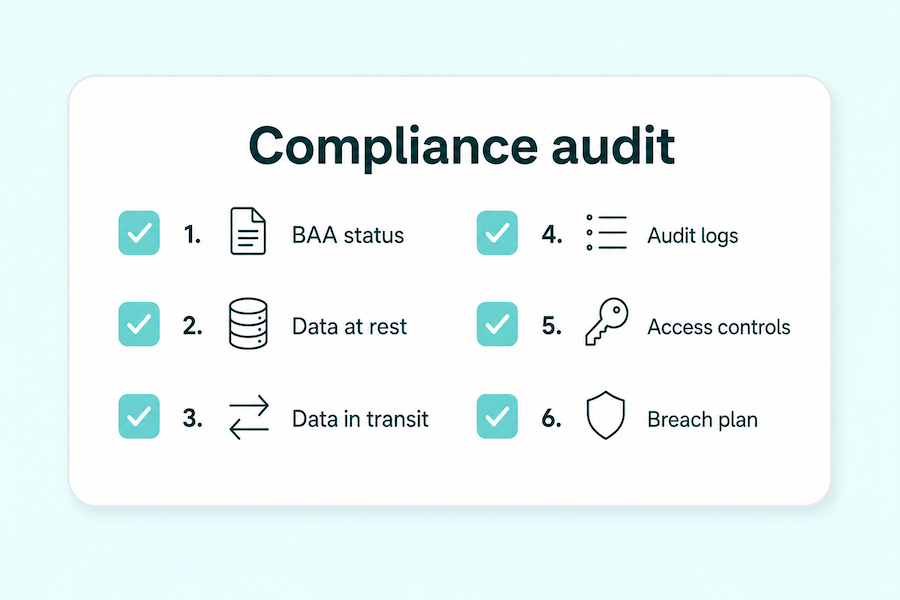
Go down the list. Answer each one for the stack you actually shipped, and ignore the tidy version in your head. Six areas:
- BAA status. Have you signed a BAA with every vendor that touches PHI? Answer this one vendor by vendor; a blanket yes covers nothing.
- Data at rest. Is PHI encrypted in your database, or is it sitting there in plaintext?
- Data in transit. Is every endpoint behind TLS, including webhooks and the admin routes you forgot you exposed?
- Audit logs. Do you have an audit log showing who opened which patient record, and when?
- Access controls. Are permissions role-based with MFA enforced, or can any logged-in account see everything?
- Breach-notification readiness. Is there a written plan for the 60-day notification clock, ready before you need it?
Each one has a pass mark. For data encryption, that's AES-256 at rest and TLS 1.2 in transit. Access controls means role-based permissions with MFA enforced, and audit logs means tamper-proof trails you can't quietly edit after the fact. That's the baseline from sprint one, and a serious health app security audit checks all of it, plus penetration testing if you want to find the holes before OCR does.
Number 6 is the forward-looking one: have the plan ready before you need it. If PHI already moved through your app without these controls, the HIPAA Breach Notification Rule's 60-day clock from discovery may already be running, which is a question for counsel.
Number 1, BAA status, is one line on this list and a whole section of its own; we get to the vendor chain shortly. The six also map to the gaps a no-code launch almost always ships with: the platform handled the easy parts and quietly left the rest to you. Worth a screenshot. And if you're building something new alongside the fix, our guide to HIPAA compliance in no-code development covers getting all six right from the start.
What OCR actually fines you for
OCR cites these exact gaps, over and over. Risk analysis, the formal risk assessment the Security Rule requires, is the single most-cited deficiency in its investigations, and has been for years. Skip it and it's usually the first thing they find, with the rest of the audit flowing from there.
The other half is unglamorous infrastructure hygiene. OCR's own January 2026 cybersecurity guidance called out default credentials left on databases, service accounts left running long after the software that used them was deleted, and patching treated as a one-time event instead of an ongoing job. None of it is sophisticated, and all of it shows up in real investigations. It's what gets skipped when you're racing to a working demo.
Platform-specific gaps: what actually breaks on Bubble, Lovable, and your no-code stack
Your backend can be made compliant. But your backend is only one layer of the app, and the layer the gap actually lives in is usually higher up. Each part of the stack covers something different, and what it leaves uncovered is where PHI leaks.
Builder layer vs data layer
Split the stack in two. The builder layer is Bubble, Lovable, or similar tools. Underneath sits the data layer: Supabase, Firebase on Google Cloud, or Airtable. The database can almost always be brought under a BAA; the builder layer often can't, and that's where the gap sits. Teams keep fixing the layer that was already fixable. So if you're scoping Bubble health app HIPAA remediation, start at the builder.
Who offers a BAA, on what plan, covering what
Two points. Lovable ships no BAA of its own, so a Lovable health app HIPAA fix means auditing Supabase and Clerk underneath. Supabase HIPAA support and Firebase HIPAA support are both real, but neither is automatic; each needs the right plan and config first. Our guides to Bubble and HIPAA compliance and Lovable's HIPAA gaps go deeper.
Where coverage actually stops
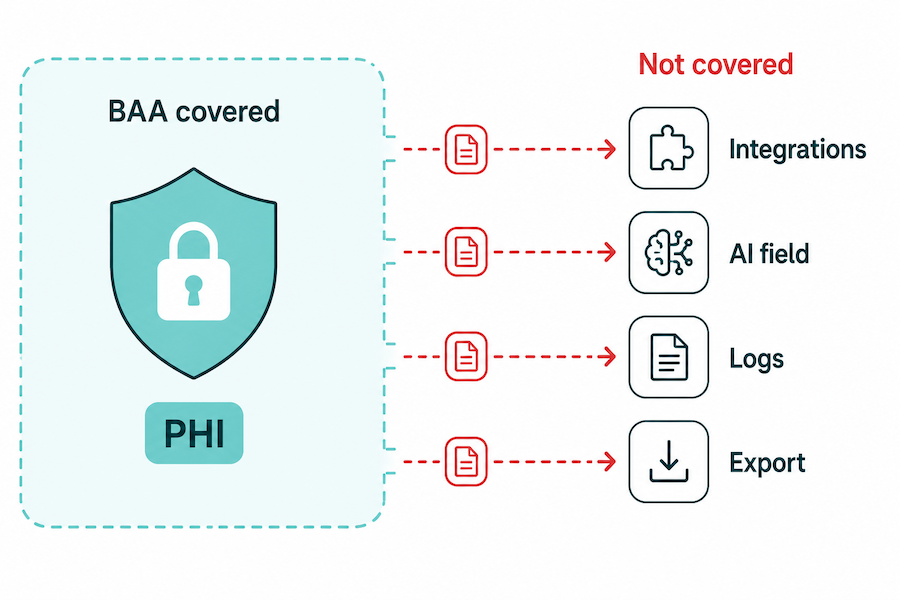
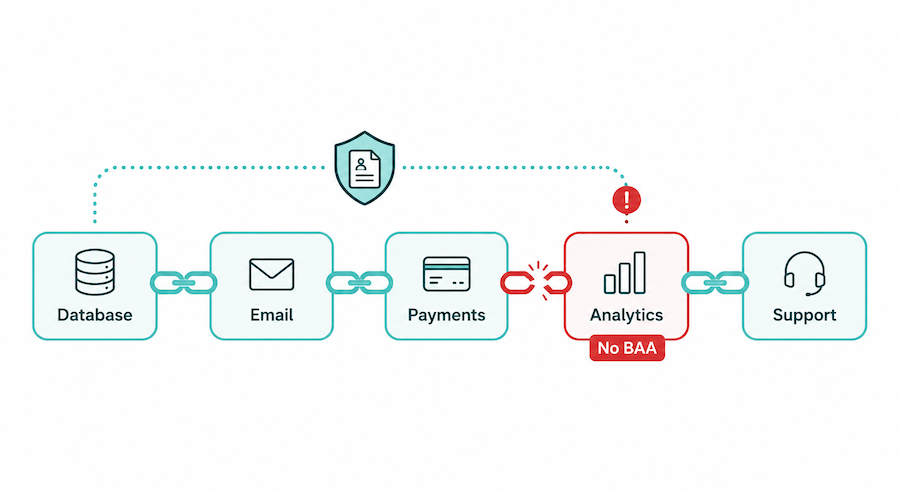
Even a fully contractable backend leaks at one boundary. The BAA covers PHI inside the database. The moment that data flows somewhere the BAA never named, a Zapier or Slack integration, an AI field, an error log, a prompt, or a CSV export, you're outside coverage. That boundary is where most no-code health apps break, and it's exactly Airtable's failure mode, which our Is Airtable HIPAA compliant? piece breaks down.
The vendor chain problem: every tool that touches PHI needs a BAA
HIPAA compliance is a chain of trust that runs through every tool touching PHI, your database included. A health app live without BAA coverage on even one vendor is non-compliant, no matter how locked-down the rest of the stack is. One missing link breaks the whole thing.
The vendors you forgot touch PHI
Beyond the database, PHI flows into tools you set up in five minutes and never thought about again:
- Email and transactional mail: appointment reminders and password resets carry PHI.
- Analytics: page URLs and event data leak diagnoses and visit context.
- Error and crash trackers: stack traces capture whatever sat in memory, patient records included.
- Payment processors: billing ties a name to a service.
- Customer-support tools: a ticket is full of PHI the second a patient describes their problem.
- Messaging and comms: chat and SMS both carry it.
A business associate agreement is what lets the electronic protected health information in your app legally reach a vendor, and the obligation flows down to that vendor's subcontractors too. Missing or inadequate BAAs are among OCR's most-cited violations. The full mechanics are in our piece on what a BAA is and who needs one.
What happens when you skip a BAA
Two companies show what skipping this costs. GoodRx paid the FTC $1.5M in the first-ever Health Breach Notification Rule action, after a Meta Pixel and a handful of SDKs quietly sent prescription and telehealth data to Meta, Google, and Criteo, plus Branch and Twilio. One month later, BetterHelp paid $7.8M for funneling intake-questionnaire answers to ad platforms for targeting.
The part that should worry you: neither GoodRx nor BetterHelp was a covered entity. The FTC enforces consumer-privacy law where OCR's HIPAA authority doesn't reach, so "I'm not technically a covered entity" buys you nothing. The PHI exposure health app fix is the same either way: a signed BAA with every vendor in the chain, and no PHI moving anywhere one isn't already in place.
The pattern is expensive at scale. Pixel-tracking penalties across healthcare now top $100M, including Advocate Aurora at $12.25M and Mass General Brigham at $18.4M, almost always traced back to poor vendor oversight.
The bar is about to rise
This bar is rising, though the timeline is uncertain. If the proposed 2026 Security Rule finalizes, a signed BAA on its own would stop being enough: vendors would have to verify their safeguards every year, with written analysis and certification.
The direction of travel is paperwork to evidence, from "we have a contract" to "prove the controls are real." That shift is coming whether or not this particular rule survives, so building the vendor chain to that standard now is the safe bet.
Triage: your 30-day remediation plan vs. what needs a migration
Not every gap is equal. Going from MVP to production with real patients turns config oversights into liabilities overnight, and the instinct is to fix everything at once. Sort first. Before you try to fix HIPAA compliance health app problems in a single frantic sprint, split them: quick wins on one side, structural problems on the other.
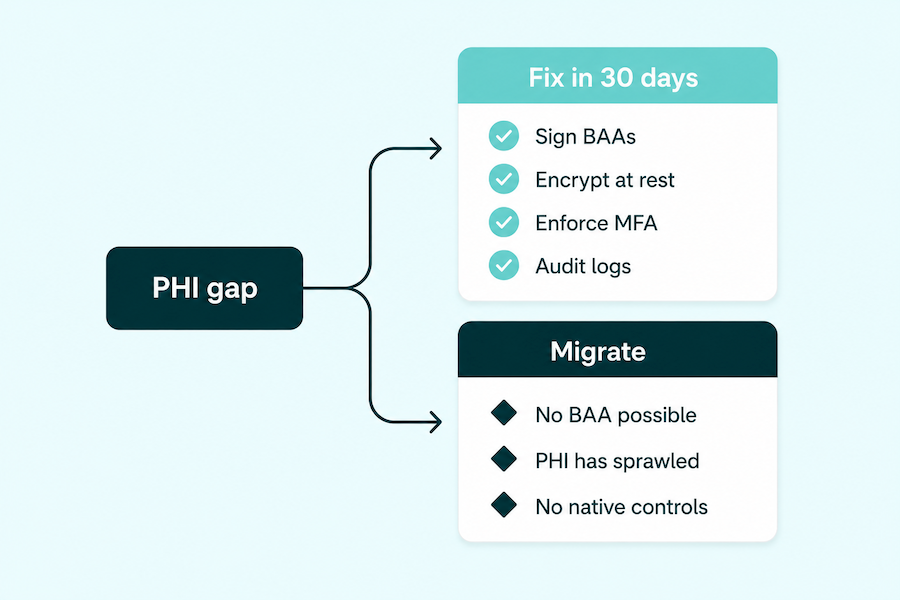
Quick wins: fix these in the next 30 days
These are in-place fixes. Numbered so you can work them in order:
Week 1, contracts and locks:
1. Sign BAAs with every contractable vendor. Work the matrix from the last section; every tool that can sign one, gets one.
2. Turn on encryption at rest. AES-256 on the database, so a leaked backup isn't a leaked patient record.
3. Enforce MFA on every account. Especially admin and provider logins, the ones actually worth stealing.
Weeks 2 to 4, access and visibility:
4. Move to role-based access. A patient sees only their own data; staff see only their scope. No more blanket logins where everyone reads everything.
5. Switch on audit logging across the stack. Every read of patient data recorded, so you can answer "who saw this record, and when" before anyone asks.
None of these require leaving your platform. They close the gaps your config left open, which is the distance between a working app and a defensible one. Most teams clear the whole list in under a month. Do them even if a migration looks likely; they cut your live exposure while you decide, and the work carries over to wherever you land.
Structural issues: flag these for the migration call
Some gaps a toggle can't close. PHI remediation splits cleanly here: if any of the following is true, the platform itself is the problem.
- PHI lives in a builder layer that can't get a BAA. No contract, no legal basis for the data to sit there, and no setting that changes it.
- PHI has already sprawled into logs, backups, and exports. Once it's copied into places you don't fully control, turning on encryption today doesn't un-spread yesterday's data.
- You can't enforce RBAC, audit logging, or encryption natively. If the platform has no real way to do these, you're bolting on workarounds that won't survive an audit.
If any of these is you, you're facing a migration decision, and the next section is the go/no-go for making it.
When patching isn't enough: signs the platform itself is the ceiling
One test decides this. Can the layer holding your protected health information be put under contract (a BAA) and under control (real access rules, logging, encryption)? Whether no-code is "good" or "bad" doesn't enter into it. If the answer is no, patching is rearranging deck chairs, and the honest version of healthcare app compliance remediation is a migration.
The signals that say migrate
Four questions settle it, and the answers are usually clearer than you want them to be. A "no" on any of the first three, or a "yes" on the last, means the platform is the ceiling and you migrate:
- Can the layer holding PHI sign a BAA?
- Can you enforce role-based access and audit logging on it natively?
- Can you encrypt PHI at rest and in transit on this layer?
- Has PHI already spread into logs, backups, or exports you can't fully purge?
If you landed on a migrate answer, the temptation is to argue with it, to find the one workaround that saves the rebuild. Sometimes there isn't one. The reasons are physical, and there are two that matter.
Start with the one founders most underestimate: shared data can't be recalled. Once PHI has been shared or leaked, you often can't fully remove it, and the receipts are blunt:
- The FTC has flagged the inability to fully remove personal data once it's been shared.
- GoodRx's data, once it reached Meta and Google, couldn't be clawed back.
A data breach behaves the same way. Once your records are loose in someone else's systems, you don't get them back.
The second reason is quieter. In a non-BAA environment, PHI copies itself into places a later toggle can't reach:
- application logs
- nightly backups
- CSV and data exports
- whatever third-party tools you wired in
Most of those copies stay invisible until an auditor or an incident surfaces them, which is why "we'll lock it down later" rarely holds. By the time you try, the data's already in a dozen places. We make the fuller case in the trap of no-code in healthcare.
The economics of waiting
The math only gets worse with time. Retrofitting compliance after launch runs about 3 to 5 times what building it in from the start costs, and that multiplier climbs as PHI exposure spreads further into your stack.
Every month you spend patching a platform that's already failed the test above is a month that makes the eventual move more expensive and the cleanup bigger. There's a version of this where you wait two quarters, wire in more integrations, and multiply the surface you'll eventually have to migrate. If the test says migrate, the cheapest day to start is today.
How to migrate without taking your app offline
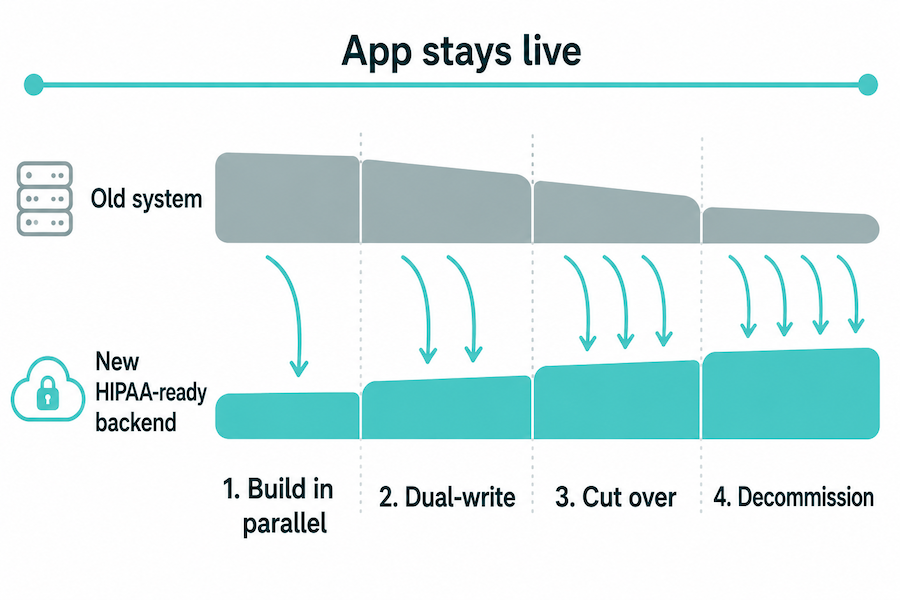
You don't have to take the app down to get compliant. The move is to build the safe version alongside the live one and shift PHI over in controlled steps, so users never see an outage. That's how to become HIPAA compliant after launch without a maintenance window or a big-bang rewrite.
The parallel-build playbook
A HIPAA compliant migration runs in parallel with the live app. Four steps:
- Stand up the HIPAA-eligible backend in parallel. Provision the new infrastructure with nothing pointed at it yet, so the live app stays untouched.
- Dual-write and backfill. Write new data to both systems and copy the history across, so the two hold the same records.
- Cut traffic over incrementally, and verify. Move users a slice at a time, checking each slice before the next.
- Decommission the old PHI store. Once traffic's fully moved and verified, shut the old data layer down for good.
This is the strangler-fig pattern, an established way to handle an infrastructure migration without downtime: the new system grows around the old one until the old one can be retired. Teams move production databases this way all the time, so the path is well-worn.
Through all four steps, keep patients and providers in the loop with a short note on what's changing and when, so the cutover doesn't catch anyone off guard.
Keep the UI, rebuild the rails
The shape that saves the most work: keep the parts that are working and rebuild only the parts that carry risk. Your no-code builder stays as the speed-and-frontend layer, the thing that let you ship fast in the first place, and there's no reason to throw that away. What moves to a HIPAA-eligible backend is the risk-carrying half:
- authentication and role-based access
- the data model
- audit logs
- encryption
- the vendor chain
That backend can be Supabase with a BAA, or a cloud platform like AWS, Azure, or GCP, all of which offer HIPAA compliant hosting under a signed agreement. Done this way, moving from no-code to custom development is a layer swap: you keep the product and replace its foundation, which is what makes custom healthcare software reachable on a startup timeline.
Timing decides how clean this is. Do this before PHI sprawls and you skip the logs, backups, and exports cleanup entirely, because there's nothing to clean up yet. That's the real reason to act at the threshold: migration is cheapest and cleanest while the data is still contained to one place.
How Specode gets you compliant without starting over
Getting compliant doesn't mean starting over. Specode is an AI builder for healthcare apps: hand it the spec your current platform can export, or describe the product you already built, and the AI rebuilds it on HIPAA-ready infrastructure in days rather than months, far quicker than a from-scratch rebuild.
That's what makes it a real migration partner for healthcare startup compliance. You build on a HIPAA-ready foundation from day one, so there's no compliance retrofit to pay for and none of the 3-to-5x tax of adding it later. The backend hosting BAA comes included on the Pro plan, which takes the biggest link in your vendor chain off your plate.
A built-in compliance agent scans your code for HIPAA issues you can fix before they ship, and you own 100% of that code, exportable anytime, so moving fast doesn't cost you control. Before you go live, the team reviews the build for security and HIPAA gaps, usually inside a couple of business days.
And if you're further in than patching can fix, the Custom tier puts Specode's own engineers on the build, reusing your existing sources where they can. It's priced as a subscription: even a few months of either tiers come in well under a from-scratch rebuild.
The cleanest time to do any of this is now, at the threshold, before PHI sprawls into logs and backups you'll be chasing down later. That's what already launched health app HIPAA compliance looks like when you move early: the same product your users already know, on infrastructure that survives an audit. If that's where you are, talk to us before the next patient signs up, while the migration is still cheap.
Frequently asked questions
Sometimes. Only if you move PHI off the non-BAA layer and bring the rest under contract and control. Otherwise, no.
Run the six-area audit, then triage. Week one: sign BAAs, enable encryption at rest and MFA. Flag structural gaps for the migration call.
Possibly. If PHI was exposed or impermissibly disclosed, the Breach Notification Rule's 60-day clock may apply. It's fact-specific, so consult counsel.
Quick wins land in about 30 days. Migrating the PHI layer usually runs weeks to a few months, depending on data volume and how many integrations touch it.
A Far less on a builder than from scratch. A from-scratch HIPAA MVP with a dev team runs roughly $35K to $90K; rebuilding on an AI app builder is a monthly subscription, usually a fraction of that.
No. Bubble offers no BAA, Lovable only possibly at Enterprise, and a BAA doesn't cover disclosures that already happened without one in place.