Healthcare App Prototyping: From Idea to Compliant Launch

You can describe a telehealth app in plain English and watch an AI builder turn it into a working demo before lunch. Screens, logins, a patient intake flow, all of it clickable. That capability is real, and it's changed what healthcare app prototyping looks like: building a fast, testable version of your app to validate the idea before you commit to a full build. What makes it different from prototyping in any other industry is the data. The moment a real patient record enters the picture, the work stops being a design exercise and becomes regulated.
Founders are already building this way. Rapid prototyping on AI tools is how a lot of 2026 healthcare apps start life, and much of that AI touches patient data with no compliance architecture behind it.
The catch: the same tool that handed you a proof of concept in an afternoon usually can't legally hold a real patient record. So the move is to use the right tool for each stage of the work.
The rest of this draws that line: which prototypes are safe to build, how the popular tools compare, where regulation kicks in, and how to get from a validated demo to launch.
How do you take a healthcare app from prototype to compliant launch?
Prototype on synthetic data with any fast tool, since in healthcare the trigger for HIPAA is real patient data entering the build, regardless of how polished it looks. General-purpose tools like Figma, Lovable, Replit, and Bolt are great for validating an idea, but none sign a BAA, so once real PHI enters you have to move onto HIPAA-ready infrastructure with encryption, row-level access controls, audit logs, and a BAA signed across every vendor. Prototyping directly in a HIPAA-ready tool like Specode collapses both stages into one build and skips the migration.
Key Takeaways:
- Your compliance obligations start when real patient data enters the build. You can build as high-fidelity as you want on synthetic data with zero HIPAA exposure; the clock starts the moment a real patient record shows up.
- Every general-purpose tool is great for prototyping and unusable for real PHI. Figma, Lovable, Replit, and Bolt all produce a working demo fast, but none sign a standard BAA, so none can legally hold patient data.
- The safe move is to keep real PHI out of the prototype tool entirely. Build and demo on synthetic data, and if real-derived data is unavoidable, de-identify it to HIPAA Safe Harbor first. The same rule reaches past the database to prompts, logs, and analytics.
- Going to production keeps your design and rebuilds everything underneath it. The validated UI and user flows carry over; the backend, encryption, access controls, audit logs, and BAA chain get rebuilt on HIPAA-ready infrastructure, which runs around $250,000 in the first year on a general-purpose builder.
- Prototyping in a HIPAA-ready tool skips the migration tax. Build in Specode and the prototype and the production app are the same build, so you pay the compliance bill once instead of twice.
The three prototype types, and which ones start the compliance clock
There are three kinds of healthcare app prototype, and only one of them puts you in regulated territory. Founders usually sort them by fidelity, meaning how real the thing looks and feels, from rough wireframes up to something that behaves like the finished product:
- low-fidelity mockup
- clickable prototype
- functional build
For most software, sorting by fidelity works fine.
Healthcare is the exception. How polished your healthcare app prototype is tells you nothing about whether you've picked up a compliance obligation. The variable that matters is the data underneath. Real patient data, or not.
That fidelity instinct is borrowed from consumer software, where a prototype stays a prototype until you decide to ship it. Healthcare doesn't grant that grace period.
Sort by the wrong axis and it cuts both ways. You either burn caution on a sandbox that never needed it, or walk into a violation while you still think you're just testing.
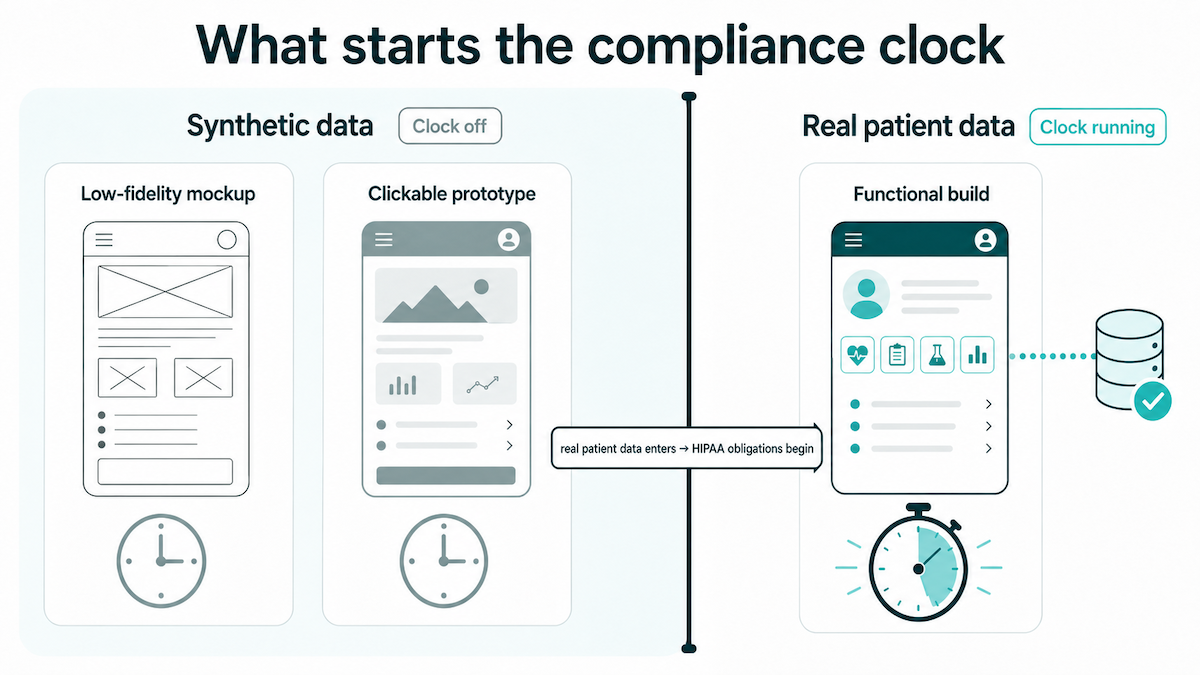
The graphic above pins down one half: which state you're in. When the clock starts is the other half.
The clock starts earlier than the go-to-production moment most founders picture. It starts the second real patient data touches the app. A throwaway mockup that leaks one real record into a live environment has started your compliance obligations just as surely as a full launch would. The data crossing the line is the trigger, nothing else.
That's the freeing part. You can build a high-fidelity prototype, wire up every screen as a fully interactive prototype, polish the entire healthcare app design, and still owe nothing to HIPAA, as long as the records underneath are synthetic. A low-fidelity prototype and a pixel-perfect one carry the same compliance weight, which is none, until the data changes.
Healthcare app prototyping tools compared: Figma, Lovable, Replit, Bolt, and Specode
All five of these tools can build you a healthcare prototype. Only one can also run it in production without a full rebuild. What separates them is a single document, and the table below makes it obvious.
Every one of them is genuinely good for prototyping
Credit where it's due: for the prototype stage, these tools are excellent. Figma is the standard for design validation and user experience work, the place you wireframe screens and pressure-test a flow before anyone writes code. When you need a clickable artifact for usability testing or an investor demo, it delivers.
The AI builders go further. Describe your idea to Lovable, Replit's Agent v4, or Bolt and you get a working frontend with the backend and database to run it, often in the time it takes to write the spec. That's a genuine shift in how fast you can build a healthcare app prototype and put something real in front of users.
If you're weighing the two most popular, we lined up Lovable vs Replit for your healthcare app separately.
Testing an interface with real users, showing investors a live product: that's most of what a prototype is for, and any AI app builder here does it well.
The shared limit: none of the general-purpose tools sign a BAA
What the four general-purpose tools have in common is one thing: not one of them signs a standard business associate agreement. No BAA means no legal path to running real PHI through the tool, however production-ready the build looks.
They each land there by a different route:
- Figma's acceptable use policy flatly prohibits PHI.
- Replit has said on the record that it offers no HIPAA-compliant hosting.
- Lovable's own terms and privacy pages tell you not to upload PHI, which is an odd foundation for a healthcare app.
- Bolt doesn't mention HIPAA anywhere in its public docs.
Same destination every time: good for a synthetic-data prototype, closed to a real patient's chart.
The comparison, and the one tool built to cross the line
Line them up on the four things that decide whether a health app prototype can grow into a real product, and the split is stark.
The Specode row is the only one that clears all four columns. Fast to build, BAA included, cleared for PHI in production, and yours to keep.
That last column, code ownership, does more work than it looks. Gil Vidals, CEO of HIPAA Vault, puts it plainly:
"If you can't export your code, you don't own your compliance destiny."
Being able to move your validated build onto compliant infrastructure, instead of rebuilding it from scratch, is exactly what ownership buys you. A tool that locks you in has quietly decided your compliance options for you.
So it comes down to one question: when real patients show up, does this tool make you start over? There's a fuller rundown in our medical app builder comparison. Answer that question honestly and the choice usually makes itself, whatever demo impressed the room.
The compliance line: when your prototype becomes a regulated product
A medical app prototype turns into a regulated product the moment real patient data enters it. That data is protected health information (PHI), anything identifiable that ties a person to their care or payment. Once real PHI is in the build, obligations attach. There are two of them, and only one is HIPAA.
The BAA trigger
The rule is blunt. Any vendor that creates, receives, maintains, or transmits PHI on your behalf has to sign a business associate agreement (BAA) with you (45 CFR 164.308(b), 164.504(e)). Without a signed BAA, there's no legal way to put PHI in that tool. That's the whole test.
Signing one doesn't make the vendor your problem alone, either. HHS holds business associates directly liable for how they handle PHI, whatever the contract says. So a vendor that won't sign a BAA is telling you something plain: it isn't built to be responsible for patient data, and neither the paperwork nor good intentions will change that. We took apart one such refusal in “Is Replit HIPAA compliant?”
The second gate: when your app is also an FDA problem
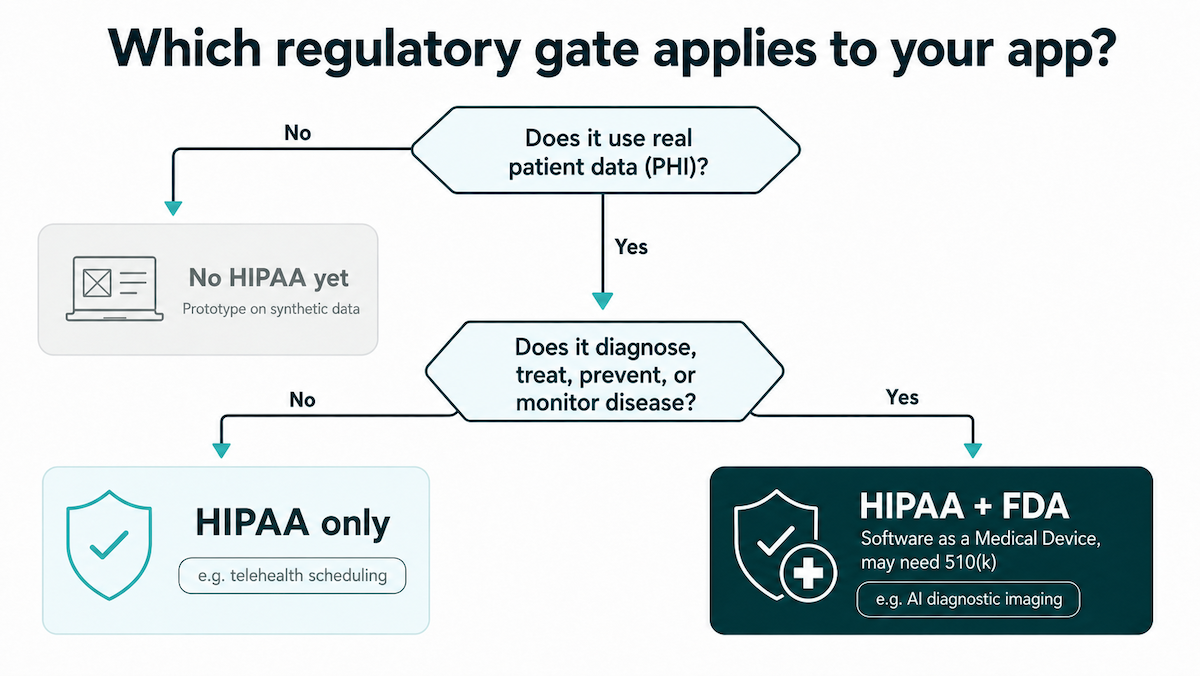
HIPAA governs the privacy and security of patient data. It says nothing about whether your software is safe to use for clinical decisions. That's a separate question, and it belongs to the FDA.
If your app diagnoses, treats, prevents, or monitors disease, it may count as Software as a Medical Device (SaMD) and fall under FDA oversight on top of HIPAA. The dividing line is what the software does:
- A telehealth scheduling app handles PHI, so it needs HIPAA and nothing more.
- An AI tool that reads diagnostic images and flags findings is making a clinical call, so it may need HIPAA plus an FDA 510(k) clearance.
Work out which gates apply to your app before the first build, because the architecture bends around that answer.
Why the line has teeth
OCR is in the middle of the first serious overhaul of the HIPAA Security Rule in about 20 years. The proposed version drops the old "required versus addressable" split that let teams treat certain safeguards as optional, so encryption, access controls, and other data security basics move toward mandatory. HIPAA compliance is tightening.
The penalties were never gentle. Willful neglect tops out at $2,177,880 per identical violation per calendar year, and North Memorial Health Care paid $1.55 million in a settlement that came down to a single missing BAA.
So draw your compliance line at the start, while it's still a design decision. Wait until your stakeholders come asking, a hospital's security team, an enterprise buyer's procurement review, and the answer is already overdue.
How to prototype a healthcare app without a compliance disaster
There's one rule that prevents almost every prototyping disaster in healthcare: keep real PHI out of any tool that can't legally hold it. Use synthetic data instead, and you can move as fast as you want. Knowing how to prototype a healthcare app safely is mostly about holding that one line, everywhere the data could leak.
The rules for safe prototyping
Rule 1: synthetic data first
Build and demo entirely on synthetic data, through every iteration. It was never real PHI, so it carries no re-identification risk and no BAA obligation, and you can gather user feedback as freely as you want.
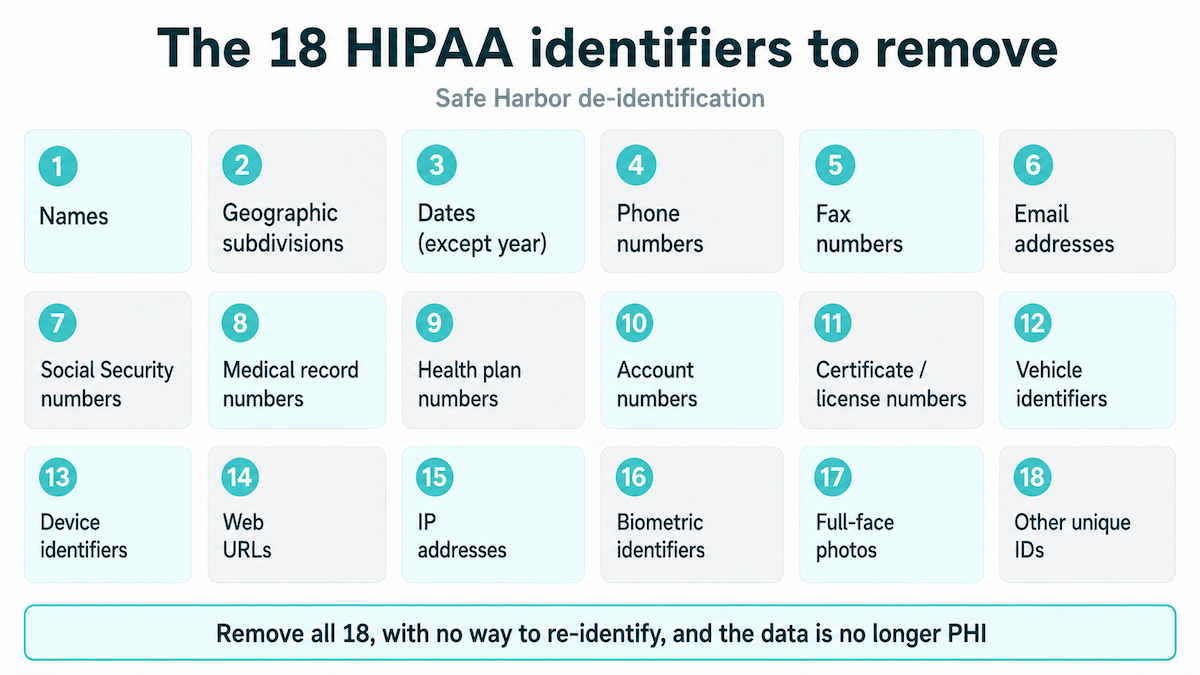
Rule 2: if you truly need real-derived data, de-identify it properly
HIPAA Safe Harbor (45 CFR 164.514(b)) means stripping all 18 identifiers and having no actual knowledge that what's left could still point to a person. Only then is it no longer PHI. Even then it carries some re-identification risk, which is why synthetic beats de-identified whenever you have the choice.
Rule 3: PHI leaks from more than the database
It's easy to lock down the database and leave the side doors wide open. Keep real PHI out of:
- the prompts and workspace artifacts you type into the AI
- debug logs and the screenshots you paste into tickets
- analytics that autocaptures fields with no BAA behind it, like PostHog or Google Analytics
None of it belongs anywhere in your development process until you're on compliant infrastructure.
The law firm Foley & Lardner, in its digital-health guidance, is blunt about the bar here: de-identification has to meet Safe Harbor or Expert Determination and guard against re-identification when datasets get combined.
The mistakes that turn a prototype into a compliance disaster
The disasters are rarely exotic. They're the same few shortcuts, over and over:
- demoing with a real patient name just to show the flow
- letting PHI land in browser localStorage
- wiring a hard delete on patient rows, when HIPAA requires you to retain them
- piping patient fields into analytics with no BAA
Any one of these can turn a clean prototype into a reportable problem.
The reason this bites harder with AI builders is that the output is often public by default and thin on security. In an April 2025 exposé, a researcher cracked Lovable-generated apps in under an hour with about 15 lines of Python, pulling out admin keys, user data, and internal AI prompts. That's the danger of vibe coding with real patient data: the demo works, and so does the attack.
Even a purpose-built preview stays synthetic-only. Specode's own preview and demo URLs are not HIPAA-compliant, which is why auth-enabled apps ship with example logins, so you test the flow on synthetic data and never a real patient.
From validated prototype to compliant launch: what actually has to change
The good news about moving to compliant production is how much of it you keep. Your validated prototype is the blueprint. What you designed carries over, and the work ahead is rebuilding what runs underneath it, on infrastructure that can legally hold PHI.
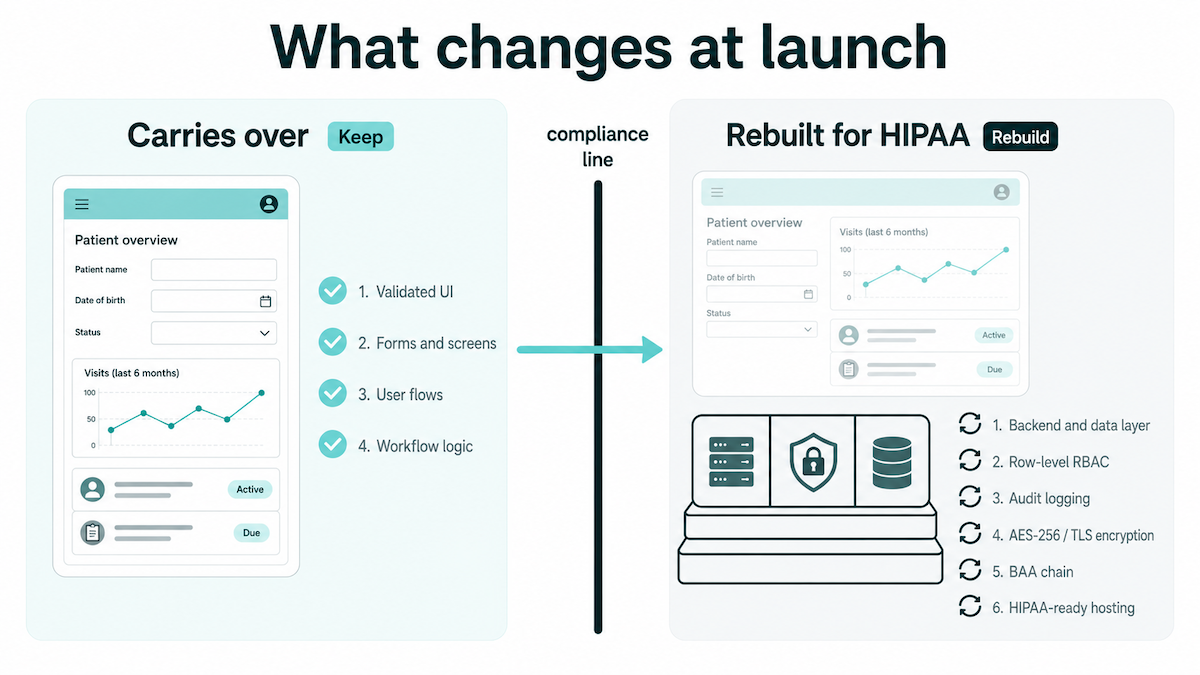
What carries over, and what gets rebuilt
Prototyping a healthcare app produces real, durable value, and most of it survives the move to production. The interface and the user flows you validated carry over intact, because that's what the prototype was actually for.
The prototype becomes your blueprint, and a blueprint is worth a lot here. It takes the guesswork out of the rebuild: you're re-implementing a product you already know works.
The rebuild is everything underneath. The backend and data layer, the whole tech stack, move onto compliant infrastructure, and the controls a prototype skips get built for real: encryption at rest and in transit, row-level access controls so one patient can't load another's chart, audit logs that hold up in an inspection, and a signed BAA with every vendor that touches PHI.
That BAA chain is rarely one signature. Vercel signs a BAA only on its Enterprise plan; Supabase only on Team plus a HIPAA add-on. Every PHI-touching vendor in your stack needs its own, and one link without a BAA breaks the chain.
The migration tax, and the lock-in that makes it worse
On a general-purpose builder, none of this is free. Getting a validated prototype to a state a hospital would accept realistically means:
- roughly 6 separate hardening surfaces
- on the order of $250,000 in the first year
- 9 to 12 months of work
We've written up what that actually involves for two common starting points: launch a healthcare app from a Replit prototype and build a compliant health app with Lovable.
The lock-in trap makes it worse. If your builder won't let you export the code, a full rebuild from scratch may be your only path forward. And once real PHI is in the picture, the export itself becomes part of your risk profile, one more place patient data can spill.
This is the real cost of healthcare app prototype development on a tool that was never built for PHI: the migration tax is the bill for using the wrong tool at the wrong stage. There's a fuller walkthrough in our guide, Lovable prototype to HIPAA-compliant health app.
What healthcare app prototyping costs, and how long it takes
Prototyping is cheap. An AI builder costs little more than a subscription and gets you a working version in hours, since AI-assisted coding runs roughly 40 to 60 percent faster than hand-building. That's the easy part. The number that actually matters is the compliance bill that lands at production, and there's a penalty for putting it off: retrofitting HIPAA after launch costs 2 to 3 times more than building for it from the start.
The cheap end is exactly the right spend. Clearstep put about $1,500 into a clickable prototype and used it to raise $400,000, which is what a prototype is for. The jump in the table is HIPAA itself: compliance adds roughly 20 to 50 percent to a real medical app prototyping budget, and an MVP that can legally hold PHI starts around $25,000 and takes 8 to 14 weeks to build.
The expensive mistake is paying for compliance twice: once by skipping it in the prototype, and again when a pilot with real patients forces the fix. Build on HIPAA-ready infrastructure from the start and that bill comes once.
That's what the bottom row shows. Specode gives you a working build in about 10 minutes and a production-ready app in 1 to 2 weeks, so the prototype and the compliant version are the same build.
How Specode takes you from prototype to compliant launch
Specode is built for exactly this. It's HIPAA-ready from day one, with auth, sane data-access patterns, and audit-friendly workflows already in place, so it's handled before you write your first prompt. The hosting BAA is included on the Pro plan, and you keep full ownership of the code with no lock-in, so the exit path is always yours.
Prototype in Specode and there's no separate migration step, so you skip the migration tax completely. The prototype you validate with users is the same build that goes to production, hardened and hosted. Same prototyping speed, with no second compliance bill and no rebuild at production.
Under the hood, it's built around the clinical workflows healthcare providers actually run, with the pieces you'd otherwise bolt on yourself:
- a built-in HIPAA Compliance Agent that scans your code for violations
- access controls, audit logging, on-demand pentesting and MFA through Maestro
- a pre-go-live security review by the Specode team
- EHR integration and eRx for when the prototype grows up
So if you're about to prototype a healthcare app, start it on infrastructure that can carry it all the way from first demo to compliant launch, with no migration project waiting on the other side. Start building with Specode.
Frequently asked questions
Both work well for synthetic-data prototyping and design validation. Neither can legally hold real PHI, though, because neither signs a standard BAA.
Not while it runs on synthetic or de-identified data. The moment real patient data enters, HIPAA applies and the prototype does need to be compliant.
On an AI builder, little more than a subscription. An agency clickable prototype runs roughly $1,500 to $40,000, depending on scope and fidelity.
Hours to a few days on an AI builder, and about 10 minutes for a first Specode build. An agency clickable prototype takes a few weeks.
Before any real patient data is involved, meaning before a pilot with real patients. That's when a BAA and HIPAA-ready infrastructure become mandatory.