How to Build a Speech Therapy App in 2026

Speech therapy mobile app development is a sequencing problem. We've watched teams pick a tech stack before picking a clinical category, then pay for it in compliance prep, ASR retooling, rebuilt go-to-market plans, and another 6 months of runway.
Founders and product teams shipping these apps are the audience here; healthcare providers shopping for an app to deploy will find better fits in vendor reviews.
How do you build a speech therapy app in 2026?
Sequence 7 decisions in order: clinical category, intended-use claim, pediatric vs adult, ASR architecture, cross-platform vs native, B2B vs D2C, and custom vs builder platform. Category and claim determine the regulator (HIPAA plus potentially FDA SaMD, COPPA, or FERPA), the ASR pick (Whisper hallucinates on aphasic speakers, so the 2026 alternatives matter), and the cost band ($40K MVP to $450K+ enterprise). Specode wins the MVP and mid-range bands; custom architecture wins the enterprise band where category-specific complexity demands bespoke build from week 1.
Key Takeaways:
- Pick the clinical category before anything else. Six clinical categories (AAC, articulation, fluency, language development, voice/aphasia, cognitive communication) each carry different regulators, buyers, ASR stacks, and cost bands. The category chosen honestly at the start determines every later decision in the build.
- The intended-use claim is what triggers compliance scope. An articulation app sold as "practice tool" stays outside FDA SaMD; the same app sold as "treats childhood apraxia" lands in Class II. HIPAA is the floor; FDA, COPPA, and FERPA stack on top by claim and audience.
- Whisper is the wrong default for speech therapy ASR. Whisper hallucinates on aphasic speakers during long pauses (~1% of transcriptions, 38% containing explicit harms per ACM FAccT 2024). The 2026 alternatives (Voxtral Transcribe 2, Deepgram Nova-3, ElevenLabs Scribe, on-device WhisperKit) are better fits depending on clinical category.
- Build for adoption; decorate with demo. Face filters and gamification close demos. In-session SLP data capture, treatment-plan integration, and caregiver tools drive clinical adoption 6 months later. Weight the build budget accordingly.
- Cost falls in three bands; the platform pick is band-driven. $40K-$80K MVP, $80K-$200K mid-range, $220K-$450K+ enterprise. Healthcare app builder platforms like Specode win the first 2 bands on time-to-market and TCO; custom build wins the enterprise band where category-specific complexity demands bespoke architecture.
Speech therapy software primer
A speech therapy app is software that delivers practice exercises, augmentative communication, or clinician-led therapy across six clinical categories: articulation, AAC (augmentative and alternative communication), fluency, language development, voice and aphasia, and cognitive communication. The apps ship on mobile or web, run cloud or on-device, and extend what speech language pathologists do in session.
The speech therapy app market: where the white space is in 2026
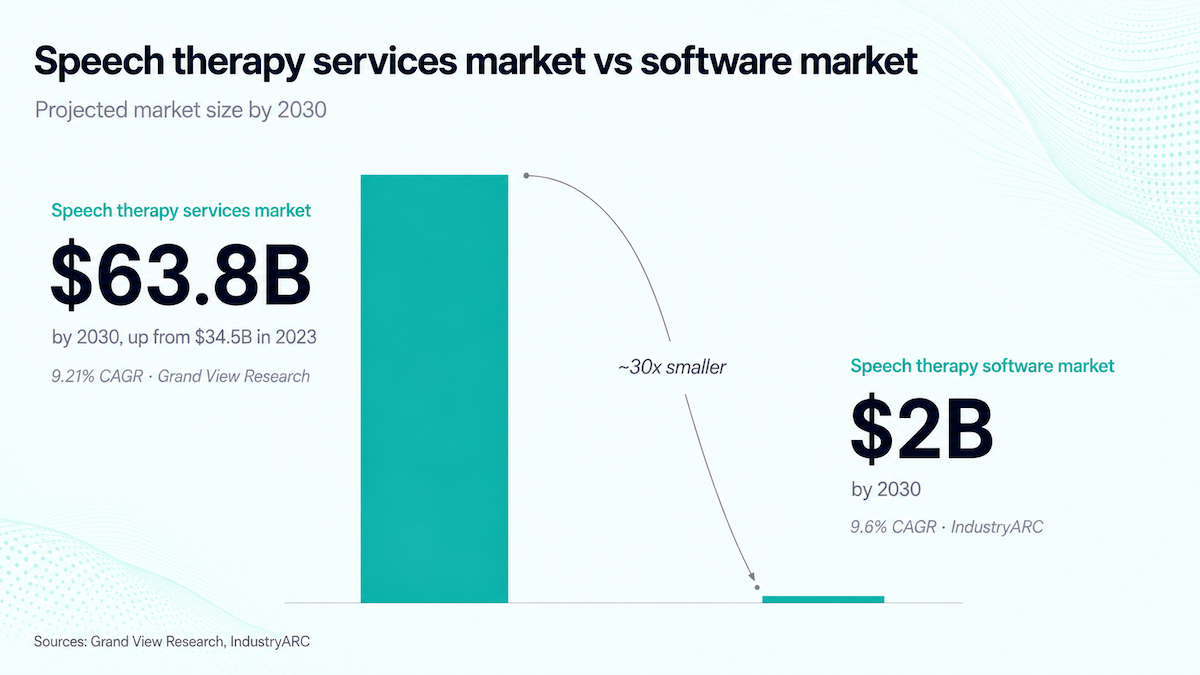
The $34-64B numbers in industry reports are the speech therapy SERVICES market, mostly physical clinics and the SLP labor that staffs them. The speech therapy software market that "how to create a speech therapy app" actually addresses is roughly $2B by 2030 at 9.6% CAGR per IndustryARC. Anchor TAM on the software figure: services shows demand depth, software shows addressable app revenue.
Demographic weight concentrates in pediatric and neurological segments. Pediatric speech therapy carries 62.77% of services revenue per Grand View (2023). Neurological conditions are the fastest-growing segment through 2030. Translated to apps:
- pediatric has demand depth and a crowded center;
- adult speech rehabilitation for neurological cases has the thinnest digital tooling and the fastest demographic growth.
The 2026 freshness anchor is the ASLP-IC. The Audiology and Speech-Language Pathology Interstate Compact began issuing privileges in October 2025, with 37 jurisdictions enacted.
A single compact privilege now replaces separate state licenses across participating states, letting SLPs run teletherapy sessions across state lines. Virtual care platforms within speech therapy services are growing at 6.78% CAGR through 2030 (Mordor).
Three openings worth a 2026 build: pediatric speech therapy apps that solve clinical workflow before chasing engagement, adult speech rehabilitation apps that target the neurological-conditions growth segment, and teletherapy app development that the ASLP-IC's cross-state privilege now enables. The crowded center (general articulation drill apps) isn't the opportunity.
Six categories of speech therapy apps (and why your category drives every later decision)
The phrase "speech therapy app" covers a fragmented market with six distinct clinical categories. To develop a speech therapy application, founders pick one of those categories at the start, and that pick drives every later decision: regulator, buyer, tech stack, cost band.
Why the category framing matters
Competitor articles default to "Top N speech therapy apps" lists. We don't, because the market isn't one market. The six clinical categories serve different populations, sell to different buyers, answer to different regulators, and need different speech recognition stacks.
Some apps span multiple categories (Lingraphica TalkPath Therapy covers aphasia and cognitive communication together), but that blurring doesn't undermine the framing. Pick the category honestly at the start, or pay for it later.
The six clinical categories
The categories, with one named clinical anchor each:
Category choice ripples through every later decision. An augmentative communication app falls under FDA scrutiny as a Class II speech-generating device. Pediatric categories (articulation therapy, language development) trigger COPPA, and FERPA stacks on top when the app sells through school districts.
Adult categories typically need HIPAA only, though most need clinician-supervised workflows that change the UX from solo-user to dual-user.
Sales motion is category-determined too. Pediatric apps sell D2C to parents (Speech Blubs) or B2B through school districts (Articulation Station). Adult apps split between D2C (Stamurai) and clinic licensing (Lingraphica).
Adjacent apps that aren't clinical
Speeko and Speechify show up on "best speech therapy apps" roundups when they shouldn't. Speeko is an AI public-speaking coach that scores pace and filler-words during interviews and presentations, a business-communication tool with no clinical claim.
Speechify is a text-to-speech accessibility tool for reading. Buyers, regulators, and success metrics don't overlap with clinical speech therapy. When you size TAM for creating a speech therapy app, drop them from the competitive set before benchmarking.
Speech therapy app features that drive clinical adoption (and which look good in demos but don't)
Speech therapy app features cluster into 2 groups, and they overlap less than founders hope. Gamification and face filters earn the wow in SLP pitches; in-session data capture and treatment-plan integration earn the renewal 6 months later. Both clusters matter to a speech language pathology app, but the build budget should weight one of them.
Demo features: the cluster that closes pitches
Speech Blubs and Otsimo lead with the engagement layer, and they're right to. Pediatric users won't sit through articulation drill 47 if there's nothing visually rewarding. The demo cluster includes face filters, gamification with point systems and unlockables, video modeling, voice recognition reactions, and real-time pronunciation feedback that color-codes accuracy. These earn the wow in a 20-minute SLP demo and photograph well in App Store screenshots.
The trap is over-indexing. The demo cluster doesn't drive the renewal decision, because the SLP wasn't the user who needed engagement features.
Adoption features: the cluster that earns renewals
Adoption-driving features serve the SLP's clinical workflow. In-session data capture for clinical documentation. Custom treatment plan creation per client. Between-session caregiver and family practice tools.
Patient progress tracking designed for SLP record-keeping rather than parent-facing dashboards. Articulation Station's in-session data collection is why SLPs use it during group therapy. Lingraphica TalkPath supports clinician-built custom plans plus caregiver tools, which is why it has staying power in aphasia clinical settings.
Build for adoption, decorate with demo
Weight the build budget toward the adoption cluster. The demo cluster decorates and engages but doesn't drive the renewal economics that determine whether the app survives year 2.
Accessibility (WCAG 2.2 AA at minimum, plus the specific needs of nonverbal and aphasic users), on-device AI inference, and multimodal AI sit underneath both clusters and serve both at once.
If the budget binds at the MVP band, cut into the demo cluster first. A featureless adoption-only app loses pediatric users; a feature-rich demo-only app loses SLPs.
Speech recognition is your make-or-break technical bet
OpenAI's Whisper API became the default AI speech recognition pick for any AI speech therapy app in 2024. It breaks where speech therapy users speak: short utterances, long pauses, atypical speech, child voices. Speech therapy app developers in 2026 have more options than the Whisper monoculture suggests.
The Whisper trap
Koenecke et al., "Careless Whisper" (ACM FAccT 2024) tested Whisper on AphasiaBank data. Roughly 1% of transcriptions contained entire hallucinated phrases. 38% included explicit harms (violence, false authority, inaccurate associations).
The hallucinations skewed to speakers with aphasia during long non-vocal pauses, the modal speech pattern in adult therapy. On the same 187 audio segments, Google, Amazon, Microsoft, AssemblyAI, and RevAI produced zero comparable hallucinations.
OpenAI itself warns against Whisper in "high-risk domains". Nabla deploys a Whisper-based tool at Children's Hospital LA and 40 other US health systems anyway, transcribing roughly 7 million medical visits.

The 2026 ASR alternatives
The post-Whisper lineup:
- Voxtral Transcribe 2 (Mistral, Feb 2026, Apache 2.0): 5.9% avg WER on FLEURS vs Whisper's 7.4%, streaming, 13 languages
- ElevenLabs Scribe: 99 languages, beats Whisper Large V3 on FLEURS and Common Voice
- Deepgram Nova-3: ~450ms median streaming latency at $0.0043/minute
- Qwen3-ASR: the top open-source pick as of early 2026
- AssemblyAI Universal-2 and Gemini 2.5 Pro: audio-intelligence features on solid WER baselines
Whisper itself still posts 2.8% WER on LibriSpeech clean. The natural language processing layer that consumes the transcript matters just as much for clinical features. The speech therapy fit is where Whisper specifically breaks.
On-device is the 2026 default
In 2026, on-device ASR is the baseline; cloud is the escalation when on-device can't handle a specific feature. Privacy expectations and the latency floor moved.
On iOS, WhisperKit and Apple SpeechAnalyzer deliver 2-8% WER on clean English audio entirely on-device using the Neural Engine (shipping since iPhone 8). On Android, createOnDeviceSpeechRecognizer() landed with API 33, and ML Kit GenAI Speech Recognition handles on-device AI inference.
Cloud ASR adds 50-300ms of network latency before inference starts, up to 2 seconds on bad connections. For wearable integration and edge deployments, Moonshine by Useful Sensors ships at 27MB.
Kids' speech is its own problem
Off-the-shelf ASR breaks on child voices, Whisper included. Higher fundamental frequency, shorter vocal tract length, immature articulation, variable pronunciation, and frequent disfluencies all push kid speech outside adult acoustic models.
The fix is fine-tuning with child-specific audio. The Ohio Child Speech Corpus (303 children ages 4-9) is the open-access benchmark. For pediatric apps, custom fine-tuning is a real cost-and-time line item that generic "build a speech therapy app" guides skip past. Expect it in the enterprise cost band.
Pick deliberately by category
ASR choice runs by category:
- AAC apps may not need ASR at all; symbol selection drives the interface
- Aphasia and cognitive communication apps need an ASR that doesn't hallucinate on long pauses, which rules Whisper out
- Pediatric apps need a kid-tolerant vendor, a fine-tuned model, or multimodal AI that combines audio with video for disambiguation
- Apps using voice biomarkers (Parkinson's screening, autism early detection) use a different stack: Wav2Vec 2.0 or HuBERT, per Bioengineering 2025
For teams committed to Whisper for ecosystem reasons, Calm-Whisper (May 2025) showed 3 of its 20 attention heads cause 75% of non-speech hallucinations; targeted fine-tuning gives 80%+ reduction. Useful for non-speech false-positives. Doesn't address the aphasia hallucination problem.
How to build a speech therapy app: the seven decisions that matter
Seven decisions determine whether a speech therapy app build ships on budget or burns through it. They sequence; they don't run in parallel. Decisions 1-3 scope the build; 4-6 shape the architecture, cost band, and user experience choices; decision 7 commits the development team to a build approach. Solve them in order.
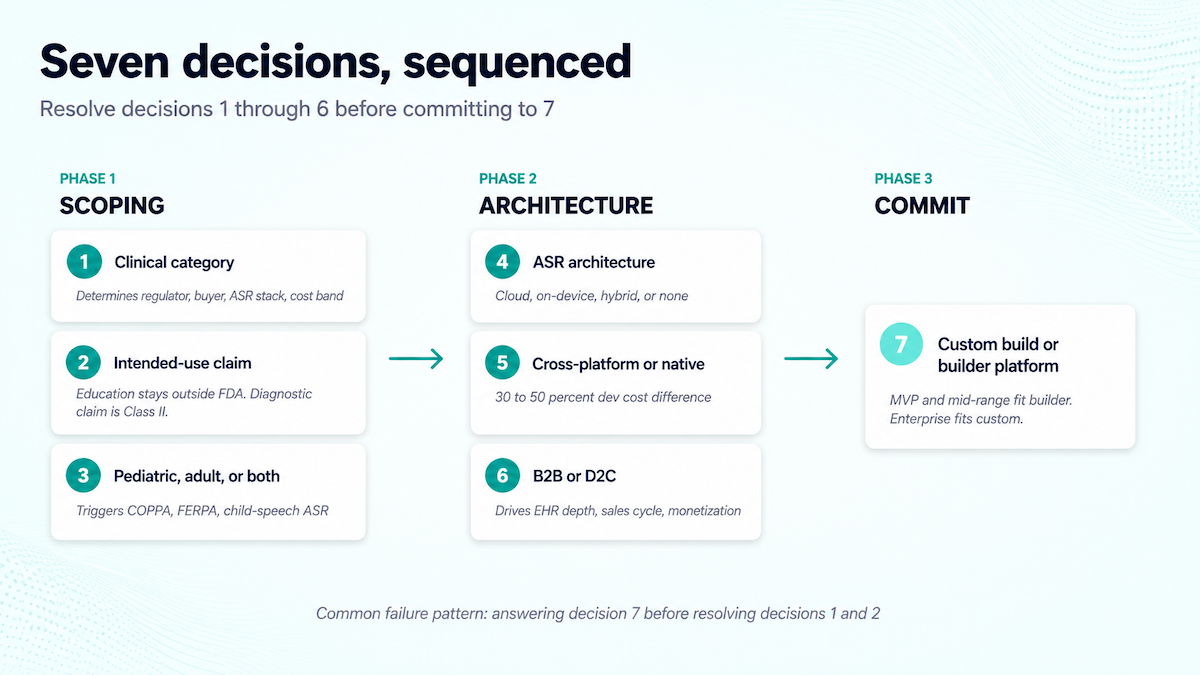
- Which of the six clinical categories are you building for? Articulation, AAC, fluency, language development, voice/aphasia, or cognitive communication. The category determines the regulator (FDA scrutiny for AAC; COPPA for pediatric), the buyer (school districts, clinics, parents, individual users), the ASR stack, and the cost band. Section 3 walks the categories. Pick honestly before anything else.
- What does the app claim to do? Educational drill apps stay outside the FDA Software as a Medical Device framework. Apps that claim to diagnose or treat a clinical condition (childhood apraxia of speech, aphasia recovery) cross into Class II, which adds verification and validation, quality assurance documentation, and 510(k) prep. The 2024 FDA cleared 168 AI/ML SaMD devices, all Class II.
- Pediatric, adult, or both? Pediatric carries a stacked compliance load:
- COPPA (the 2025 amendments tightened it)
- FERPA when the app sells through schools
Plus the child-speech ASR challenges from decision 4. Adult builds mostly need HIPAA only, though adult clinical categories typically require clinician-supervised workflows. Mixed-audience apps inherit both.
- Cloud ASR, on-device, hybrid, or none? AAC apps often need no ASR. Aphasia needs hallucination-resistant ASR; pediatric needs kid-tolerant or fine-tuned models. On-device is the 2026 baseline; cloud is the escalation.
- Cross-platform or native? React Native or Flutter shave 30-50% off iOS+Android development cost. Native earns the premium when on-device ASR is core (deep Core ML or Neural Engine integration), or when the design language has to feel native to win clinician acceptance. Default to cross-platform unless ASR depth pushes you off.
- B2B or D2C?
- B2B requires EHR integration, credentialing cycles that run 8-20 weeks past dev, longer sales cycles, and per-seat licensing
- D2C requires consumer marketing budget, subscription plumbing, and parent-as-payer economics for any pediatric play
Category usually answers this. AAC and aphasia tend B2B; fluency tends D2C, with pediatric language development going either way.
- Build custom or use a healthcare app builder platform? Most teams answer this first, and that's the problem. Custom build makes sense at the enterprise cost band where category-specific complexity (FDA SaMD prep, custom child-speech ASR fine-tuning, multi-EHR write integrations, insurance-billing plumbing) demands a bespoke development process from week 1. Builder platforms like Specode win at the MVP and mid-range bands, where most speech therapy applications live.
The most common build-failure pattern is answering decision 7 before decisions 1 and 2. Category and claim determine whether a builder platform fits at all. Anyone working out how to develop a speech therapy app should start with those 2 questions.
Tech stack for speech therapy app development
Speech therapy app development reuses the standard healthcare app stack, picked for HIPAA eligibility and cross-platform efficiency. Two layers are category-specific: the ASR pipeline (Section 5) and HIPAA-eligible real-time video for telehealth app development.
Most of the stack is commodity in 2026. The 2 non-commodity layers are the ASR/voice pipeline (category drives the vendor pick) and HIPAA-eligible real-time video. Compliance plumbing (audit logging, encryption, BAA chain mapping) compounds across every vendor; ask each prospective vendor whether they sign BAAs and which subprocessors touch PHI before signing the contract.
HIPAA is necessary but not sufficient: the four regulators speech therapy apps actually face
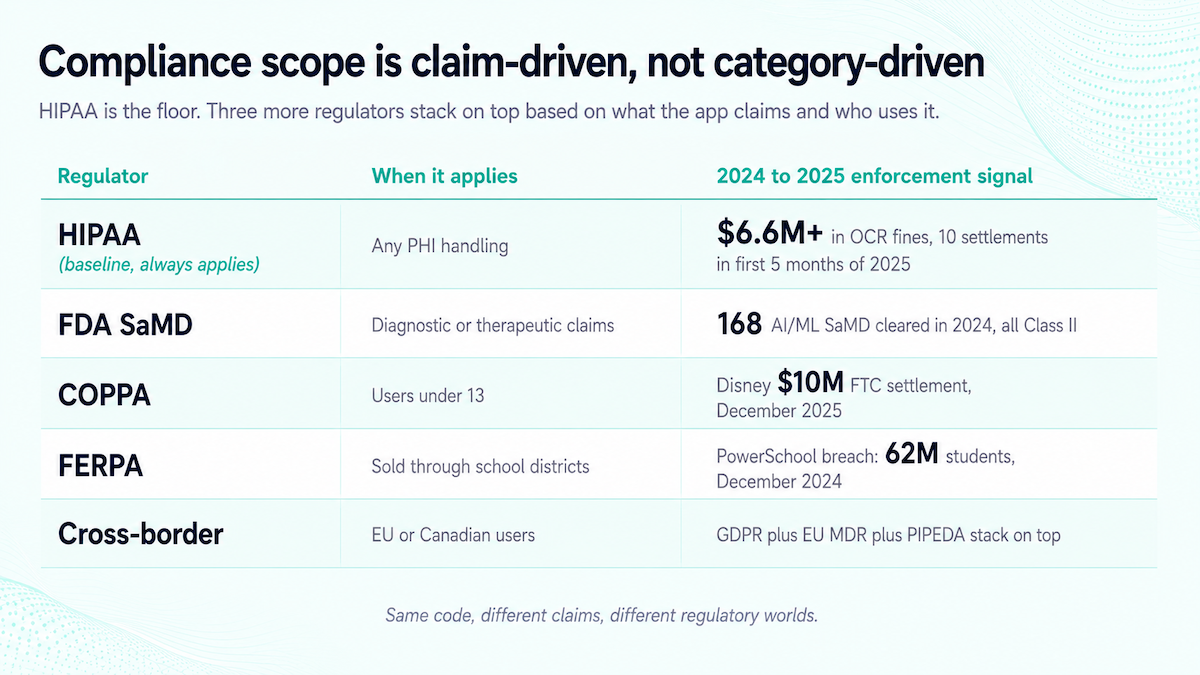
What it takes to make a speech therapy app compliant in 2026 covers 4 regulators, with HIPAA as the floor and FDA SaMD, COPPA, and FERPA stacking on top by claim and audience.
FDA SaMD: the line is your claim
FDA Software as a Medical Device covers software performing medical purposes without hardware, across 3 risk classes. In 2024 the FDA cleared 168 AI/ML-enabled SaMD devices, every one Class II. No AI/ML SaMD has been classified Class III.
AAC app development has lived in Class II territory for years (AAC devices are speech-generating devices under FDA terminology, and Medicare covers them as DME under CMS NCD CAG-00055). Educational practice apps stay outside SaMD; apps that claim to diagnose or treat a clinical condition cross in. "Practice your /r/ sound" is education. "Treats childhood apraxia of speech" is a Class II claim.
COPPA: pediatric apps after the 2025 amendments
The FTC finalized the first major COPPA overhaul since 2013 on January 16, 2025, with Federal Register publication on April 22. New requirements:
- separate verifiable parental consent for targeted advertising and third-party data sharing
- data retention limits
- biometric data restrictions
- opt-in replacing opt-out for many disclosures
Enforcement is live. The FTC settled a $10 million case against Disney in December 2025 and sued TikTok and ByteDance for COPPA violations in August 2024. Speech Blubs and Articulation Station both sit inside this zone, along with every other pediatric speech therapy app.
FERPA and the school-district sales channel
Most pediatric speech therapy apps reach kids through school SLPs, which puts FERPA in scope. The 2024-2025 breaches set the enforcement temperature: PowerSchool's December 2024 breach exposed 62 million students, and the Illuminate Education breach hit 10.1 million with plain-text storage that persisted until January 2022.
In March 2025 the US Department of Education required state agencies to certify FERPA compliance by April 30. 121+ state student-privacy laws stack on top as of 2025, including California's SOPIPA. For school-district sales, the state-law inventory is the first compliance ask in any vendor evaluation.
HIPAA: the assumed baseline, and where 2025 enforcement landed
OCR enforcement is heavier than the marketing decks suggest. 10 HIPAA resolution agreements in the first 5 months of 2025, roughly $6.6 million in fines, settlements running $25,000 to $3 million. Risk analysis is the central failure in most cases. OCR's Risk Analysis Initiative drove 7 enforcement actions in 6 months, all ransomware-tied.
Right of Access enforcement is also live. Concentra settled $112,500 in December 2025 for failing to provide patient records within the 30-day window. Being HIPAA compliant covers the 30-day rule alongside BAA signatures, data security, and risk analysis.
GDPR and PIPEDA apply for EU and Canadian users; the EU MDR substitutes for SaMD in European market entry. The same code marketed as "practice tool" versus "treats childhood apraxia" lands in different regulatory worlds. Build the compliance plan from week 1.
Cost to build a speech therapy app in 2026, and when Specode beats custom build
Cost to build a speech therapy app follows the 3 standard healthcare app development bands, sized by category, claim depth, and ASR depth.
The three cost bands
Add-ons layer on top of any band. HIPAA compliance work adds $15K-$50K. Cross-platform saves 30-50% versus building native iOS and Android separately. Twilio Video or Daily.co with a signed BAA replaces $20K-$50K of custom WebRTC build. Annual maintenance runs 15-30% of the initial build cost.
When Specode beats custom build, and when it doesn't
The build-vs-buy call benefits from years of experience in healthcare app shipping; if you don't have that in-house, a healthcare app builder like Specode wins the MVP band and most of the mid-range band on time-to-market and total cost of ownership. Custom build wins the enterprise band where category-specific complexity (FDA SaMD prep, custom child-speech ASR fine-tuning, multi-EHR write integrations, insurance-billing plumbing) demands bespoke architecture from week 1.
A white-label telehealth platform is a third option for teletherapy-heavy builds, where the video and scheduling layer is the bulk of the work and a packaged platform skips months of integration. SLP app development teams building a speech therapy app pick the path that handles the most commodity layers.
How Specode can help
The build-vs-buy decision reduces to a band question. MVP and mid-range builds get to market faster on a builder platform; enterprise builds usually need bespoke work.
Specode is built for the first case. The platform handles the healthcare app commodity layers (HIPAA compliance baseline, BAA-eligible infrastructure, authentication and audit logging plumbing, cross-platform mobile scaffolding) so the team's custom development time goes into the category-specific work that earns clinical adoption: ASR vendor integration tuned to the clinical category, treatment-plan workflows for SLPs, in-session data capture, and caregiver tools for between-session practice.
We've watched founders assemble that commodity layer themselves and lose 6 months to it, then outsource the category-specific work to a generic agency and ship features that don't earn renewal. The pattern repeats across healthcare verticals like mental health app development: outsource the commodity, custom-build the differentiation.
If you're scoping how to build your own speech therapy application in 2026 and the build sits in the MVP or mid-range band, talk to us about Specode before committing to a full custom architecture. We'll tell you honestly when custom is the right call.
Frequently asked questions
$40K to $450K+ depending on category and claim depth. MVP $40K-$80K, mid-range $80K-$200K, enterprise $220K-$450K+. HIPAA adds $15K-$50K. Cross-platform saves 30-50%.
Software delivering practice exercises, augmentative communication, or therapy support across six clinical categories. Runs cloud, on-device, or hybrid; clinical-grade products work alongside SLPs.
Automatic speech recognition (Voxtral Transcribe 2, Deepgram Nova-3, ElevenLabs Scribe, Apple SpeechAnalyzer, Moonshine for edge), voice biomarker stacks (Wav2Vec 2.0, HuBERT) for screening apps, and on-device inference via Apple Neural Engine or Android 13+ APIs. Whisper has documented hallucination risk on aphasic speakers, so the speech therapy use case rewards picking deliberately.
BAAs with every third-party processor, completed risk analysis (OCR's top 2025 enforcement focus), encryption at rest and in transit, audit logging, breach notification, and Right of Access (30-day rule). FDA SaMD, COPPA, and FERPA can stack on top.
MVP builds ship in 8-14 weeks. Mid-range cross-platform work with HIPAA takes 16-22. Enterprise builds run 28-36 weeks, plus 8-20 weeks of EHR vendor credentialing (Epic, Cerner) and 1-2 weeks of App Store and Play Store review.
No. Apps supplement clinician-delivered therapy; adoption depends on workflow fit with the SLP. Apps positioned as SLP replacements typically fail clinical adoption and trigger FDA scrutiny for unsubstantiated therapeutic claims.
React Native or Flutter for cross-platform; Node.js or Python on AWS HIPAA-eligible services; Twilio Video or Daily.co with BAA for teletherapy; FHIR via middleware for EHR; on-device ASR via WhisperKit or createOnDeviceSpeechRecognizer. Standard Zoom doesn't qualify as HIPAA-eligible.