How to Build a Behavioral Health App: A Complete Guide

Behavioral health app development looks deceptively close to a standard patient app until the first intake form touches therapy notes or substance use history. From there, the regulatory and liability load is its own animal, well past "healthcare app plus chat" territory.
You see that difference in the product backlog first. Consent logic, clinician escalation paths, analytics restrictions, EHR choices, and prescribing workflows all get more expensive once they're discovered after design approval.
The regulatory stack adds 42 CFR Part 2 for substance use records, state mental health licensing rules, FTC enforcement for apps outside HIPAA, and DEA telehealth prescribing rules that keep moving on a calendar.
The integration map gets messier too. Behavioral health workflows often run through specialty behavioral health EHRs and middleware long before anyone gets to the Epic or Oracle Health conversation.
Liability changes the build as much as compliance does. When an algorithm surfaces suicidality, duty-to-warn exposure follows. Intake flows now carry mandatory reporting obligations. And FTC adtech enforcement is what turned BetterHelp into a $7.8M settlement.
What does behavioral health app development require beyond HIPAA?
It extends into 42 CFR Part 2 for SUD records, state mental health licensing, FTC enforcement for non-HIPAA-covered apps, and DEA telehealth flexibilities extended through December 31, 2026. Realistic EHR integration is two-tier: Netsmart's CareConnect FHIR and Kipu's paid REST API.
Key takeaways
- Behavioral health app development carries five regulatory layers (HIPAA, 42 CFR Part 2, state mental health licensing, FTC enforcement, DEA telehealth), and the FTC is the most active regulator for any app not covered by HIPAA.
- BetterHelp, Cerebral, and Monument all settled over third-party tracking pixels and SDKs on screens that touched protected health data. The numbers: $7.8M for BetterHelp, $7M FTC plus $3.652M DOJ for Cerebral, $2.5M for Monument.
- Pear Therapeutics filed Chapter 11 in April 2023 because payers wouldn't reimburse digital therapeutics at drug-like rates. The post-Pear PDT pattern bundles the app with an existing clinical service.

- Realistic BH EHR integration is two-tier: Netsmart's CareConnect FHIR gives enterprise behavioral health agencies a public sandbox and self-serve registration; Kipu's paid REST API serves addiction treatment through a signed vendor agreement with no public sandbox.
- Measurement-based care moves outcomes when it uses validated instruments (PHQ-9, GAD-7, AUDIT, C-SSRS, ASRS, PCL-5), and Spring Health's published 5.6-point PHQ-9 reduction and 1.9x ROI are the marquee receipts.
- Multi-state clinician credentialing is a recurring cost line: 4 to 12 months per state for initial licensure, then renewal fees each cycle. PSYPACT, Counseling Compact, Social Work Compact, and IMLC shrink the timeline for some clinician types but never eliminate it.
Five shapes of behavioral health apps and which one you're actually building
The app shape drives the build decisions that follow. Behavioral health is broader than mental health app development because it adds substance use disorder, addiction recovery, comorbid medical-psychiatric care, and crisis-pathway logic.
Each shape carries a different regulatory exposure, integration target, reimbursement path, and unit-economics model. Most teams pick architecture first, then discover 6 months later that they built the wrong foundation for the behavioral health app project.
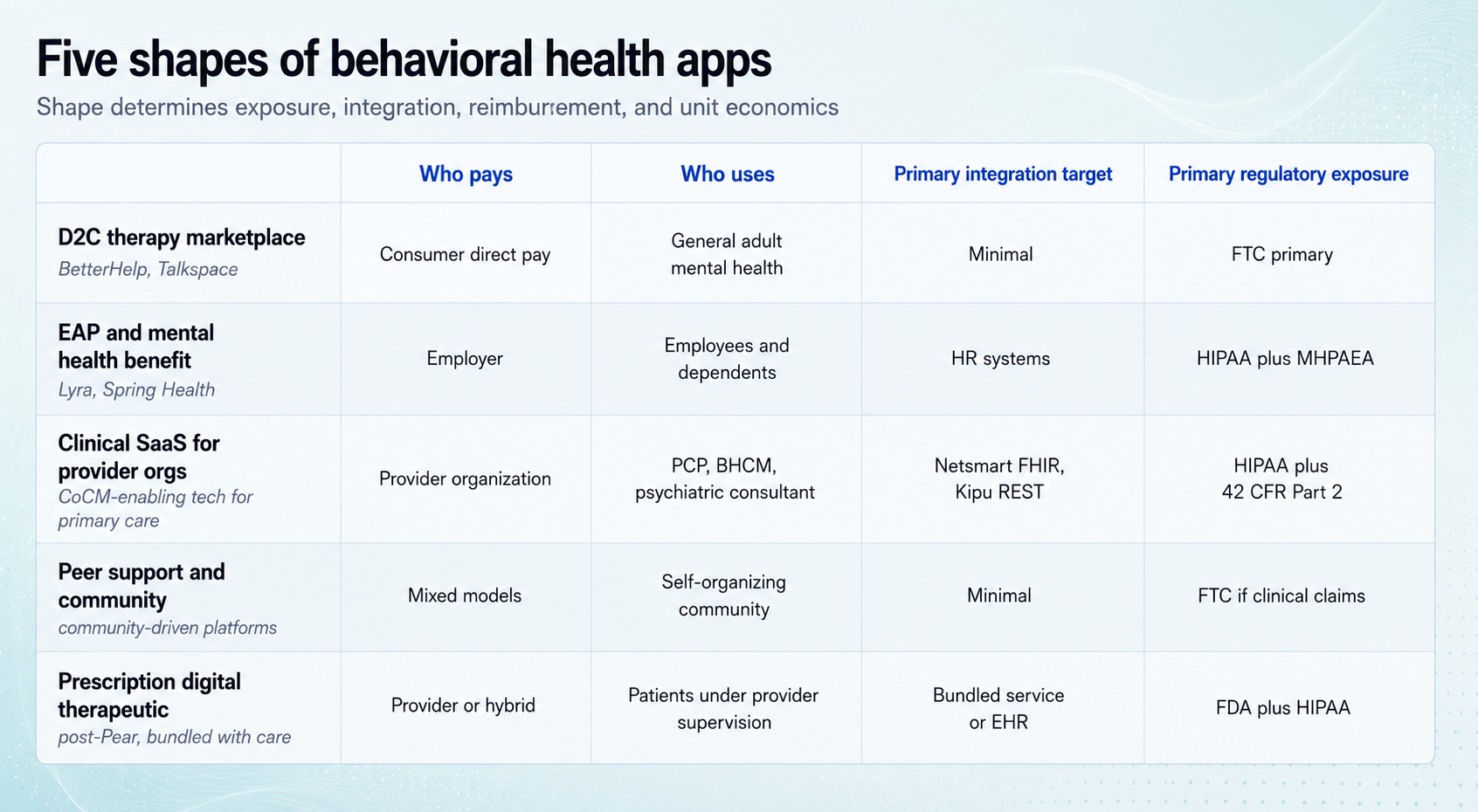
D2C therapy marketplace
BetterHelp and Talkspace set this pattern. Cerebral pushed it into telehealth prescribing before regulators caught up.
The model is simple on paper: license clinicians, acquire consumers, run subscriptions or insurance-assisted visits. The intake funnel itself can become regulated health data before the first therapy session happens.
- Who pays: the consumer, sometimes with insurance bolted on later
- Who uses: general adult mental health consumers
- Primary integration target: minimal; payment processor, EHR-lite for notes
- Primary regulator: FTC for adtech and disclosure, with HIPAA entering when the clinician's covered entity status pulls the app in
This is the highest FTC-exposure shape in 2026. The pixel-on-the-intake-page mistake costs settlement money. The FTC cases later in the post show how expensive that gets.
Employer EAP and mental health benefit platforms
Lyra and Spring Health define this shape, with Modern Health sitting nearby as a benefits-focused alternative. Employers buy the platform as a workforce benefit; employees and dependents get covered sessions, coaching, or care navigation through an HR-gated workflow.
The build has to support eligibility files, HRIS connections, dependent access, outcome reporting, and the privacy wall between employer and employee data. The regulator mix changes too. HIPAA often enters through the group health plan, while MHPAEA parity rules shape benefit design and reporting.
Lyra's 2025 outcomes-based pricing shows where this category is going: employers pay for clinical movement instead of session count.
Clinical SaaS for behavioral health provider organizations
This is the software layer for provider organizations running collaborative care management (CoCM), addiction treatment, or behavioral health programs inside a broader care model.
- Who pays: the provider organization, sometimes with health plan support
- Who uses: BHCMs, psychiatric consultants, treating PCPs
- Primary integration target: Kipu for SUD and addiction treatment, Netsmart CareConnect FHIR for larger behavioral health agencies
- Primary regulator: HIPAA, 42 CFR Part 2 when SUD records flow through, state licensure for the underlying clinical service
CoCM is the care coordination model Medicare reimburses through codes 99492 through 99494 plus G2214, around $145 per patient per month. The trap is role design. These codes only work when the psychiatric consultant stays advisory to the PCP. Once the psychiatrist starts seeing the patient directly, the billing model changes.
Peer support and community
7 Cups and TalkLife sit here. Marigold Health applies the model to substance use specifically. This shape is lighter on integration because the product center is moderated community, peer matching, escalation, and referral rather than a full clinical record.
- Who pays: a mix of consumer freemium, employer-sponsored, health-plan-sponsored, grant-funded, or some combination that looks great in a pitch deck and less great in finance review
- Who uses: people seeking peer connection ahead of or alongside clinical care
- Primary integration target: light; SSO, content moderation, optional clinician handoff
- Primary regulator: FTC if the copy promises symptom reduction or treatment outcomes; otherwise the lightest load of the five shapes
Plain peer support carries the lightest regulatory load. Once the marketing copy starts sounding clinical, the app starts sounding clinical to regulators too.
Prescription digital therapeutic
Pear Therapeutics defined this shape. Its bankruptcy reshaped the economics, and the surviving PDT pattern bundles with an existing clinical service.
- Who pays: the provider organization (addiction program, sleep clinic), with payer reimbursement as a secondary line at best
- Who uses: patients enrolled in the underlying clinical program
- Primary integration target: the parent program's EHR and billing systems
- Primary regulator: FDA (510(k) or De Novo) plus HIPAA
Pear's collapse, covered below, shows why the standalone PDT model got harder to defend.
What the leading platforms got right and where they're stuck
Platform-by-platform receipts teach behavioral health app developers more than feature comparisons do. The useful pattern usually sits in the business model, reimbursement path, regulatory action, or rollout strategy.
What Pear Therapeutics' bankruptcy told us about PDT economics
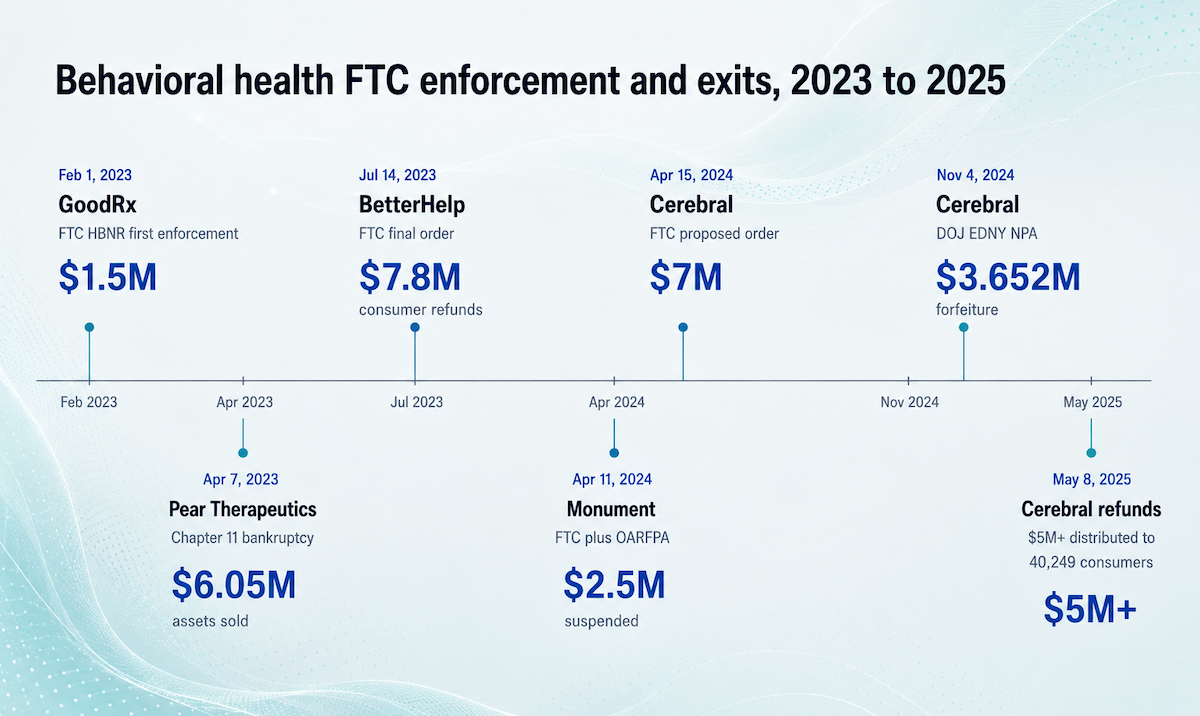
Pear Therapeutics is still the cleanest warning label for standalone PDT economics. The company filed Chapter 11 on April 7, 2023 after failing to turn FDA clearance into payer coverage at the scale the model needed.
Two receipts matter here. Pear cut 92% of its workforce, and its assets sold for $6.05M total at auction. PursueCare later acquired reSET and reSET-O, then relaunched them in August 2024 as part of its virtual addiction treatment business.
Pear's clinical case was stronger than its reimbursement path. CEO Corey McCann's own LinkedIn post named the failure mode as payer non-coverage. Almost half of Pear's revenue came from three payers with very different contract structures. A PDT priced and sold like a drug needs drug-like reimbursement to survive. The post-Pear pattern bundles the app with an existing care or business model, and PursueCare's reSET relaunch is the canonical example.
BetterHelp and Cerebral: when the FTC writes you up
Three regulator actions in 18 months hit two D2C therapy companies:
- BetterHelp: $7.8M FTC settlement (July 2023)
- Cerebral: $7M FTC settlement (April 2024)
- Cerebral: $3.652M DOJ forfeiture (November 2024 non-prosecution agreement)
The adtech lesson is direct. Intake data, hashed identifiers, ad platform audiences, and conversion events can all become health disclosures when the screen context is clinical. The HIPAA and FTC section below gets into the tracking-pixel mechanics.
Cerebral added a second lesson for prescribing workflows. The DOJ NPA described an internal "Initial Visit Rx Rate" of 95%, an ADHD stimulant rate near 100%, supervisor bonuses tied to prescribing, and a $10-per-PDMP-check policy applied only to stimulants. That is the kind of KPI dashboard that looks operational in a growth meeting and very different in discovery.
If your app nudges clinical decisions around therapy sessions or prescribing, assume the internal metrics will be read by someone outside the company one day.
Lyra: outcomes-based pricing as a maturity signal
Lyra launched outcomes-based pricing in 2025: employers pay only when clinical and financial targets get met, with a bonus if Lyra delivers and a credit if it doesn't. First commercial structure of its kind in behavioral health.
It only works because Lyra has measured outcomes for years (20+ peer-reviewed papers) and selectively credentials therapists trained in evidence-based modalities like CBT, DBT, and ACT. Spring Health publishes similar outcome data: -5.6 PHQ-9 and -5.5 GAD-7 reductions among frontline healthcare workers, plus 1.9x ROI in 2025 JAMA Network Open.
Outcomes-based pricing is what category maturity looks like. Once one platform sells against measurable clinical movement, "we connect you to a therapist" starts sounding thin.
SonderMind, Headway, and the marketplace pattern that scales
SonderMind reached all 50 states in April 2025, closing the map with New York and Michigan. Headway launched embedded primary-care EHR referrals in May 2025: PCPs can route patients to in-network therapists through their existing chart. Two Chairs took the slower path, building outcomes infrastructure before geographic expansion; by mid-2025 the company had reached 75% of the US population with employed-clinician quality controls.
Watch the payer side. Optum, Carelon, and Teladoc are increasingly building behavioral health services in-house. The marketplace pattern only scales if there's still a market when payers finish their builds.
The features that actually move outcomes
Generic behavioral health app features get downloads: chat, mood tracking, CBT prompts, meditation tracks. The features that change retention and clinical outcomes are more specific, and most apps still ship thin versions of them.
Measurement-based care is the feature most apps still half-ship
Measurement-based care (MBC) means scoring patients on validated instruments at set intervals, then using the trend to adjust treatment. Spring Health's published outcomes among frontline healthcare workers: -5.6 points on PHQ-9, -5.5 points on GAD-7 over 6 months, 69.9% achieving reliable improvement, and 1.9x ROI in 2025 JAMA Network Open.
The instruments worth implementing:
- PHQ-9: depression
- GAD-7: anxiety
- AUDIT: alcohol use
- DAST: drug use
- C-SSRS: suicidality
- ASRS: adult ADHD
- PCL-5: PTSD
These scores give clinicians and payers something sturdier than a custom mood slider. Anxiety and depression screening starts with validated tools for a reason: clinicians trust the rubric, and outcomes reporting survives review.
Crisis pathways: what happens before 988 takes over
988 has no integration API. It routes phone, text, and chat. Crisis intervention design in a behavioral health application lives in the seconds before someone dials.

The app needs a clean escalation path:
- Risk model triggers: PHQ-9 item 9 positive, C-SSRS escalation, explicit statement of intent or means
- Clinician paging: who gets notified, through which channel, with what SLA
- Documentation: what the next clinician sees in the chart
- Local resources: nearest crisis center, mobile crisis team, walk-in psychiatric urgent care, or warm handoff to a platform clinician
The FCC adopted call georouting rules in October 2024. Nationwide wireless providers are compliant; non-nationwide providers have until December 14, 2026. That helps route the call. Your app still owns the minutes before the call.
Clinician matching beats round-robin
Round-robin therapist assignment is the default in marketplaces built for speed. It also creates a bad first-session experience when the patient needs trauma expertise, evening availability, a specific modality, a shared language, or in-network coverage and gets "next available" instead.
Intentional matching should account for modality, specialty, demographics, insurance, geography, and schedule fit. Schedule fit usually does the most damage because weekday evening availability is where demand goes to fight for a chair.
Patient engagement drops fast when the first session feels wrong. Every added friction point makes the second appointment less likely.
Between-session work is where outcomes compound
Sessions are 50 minutes. The week is 10,080. The behavioral health version of remote patient monitoring lives in the gap.
Tracked CBT exercises, journaling with clinician visibility, homework completion in the chart, and mid-week outcome capture all feed the next session. The next therapy session should open on what the patient actually did between visits.
Otherwise the app is mostly a calendar with nicer typography.
HIPAA isn't your hardest problem in behavioral health
Behavioral health apps start where basic HIPAA planning runs out of road. The question of how to develop a behavioral health app safely pulls in 42 CFR Part 2, state mental health licensing, FTC enforcement for non-HIPAA-covered apps, and BH-specific liability surfaces around prescribing and crisis. Each has bitten a named platform in the last three years.
The 2024 MHPAEA final rule took effect November 22, 2024 with stricter NQTL provisions for plan year 2026, though Departments paused enforcement of the new portions in May 2025.
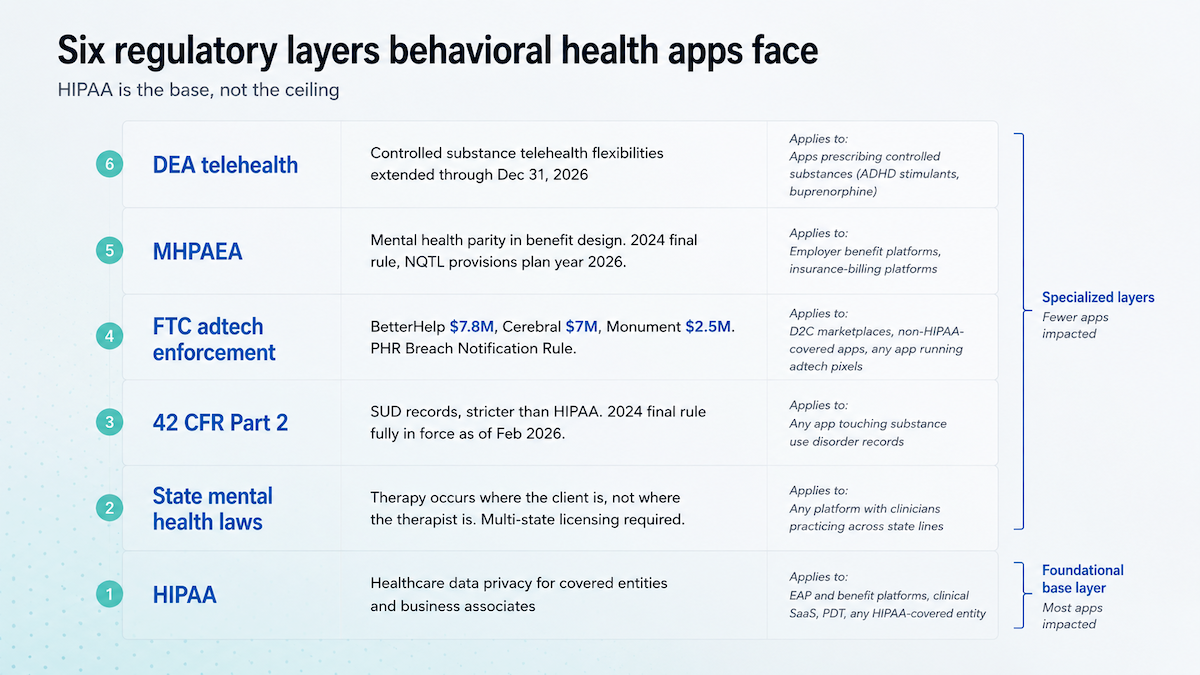
42 CFR Part 2 is stricter than HIPAA and gets confused with it
42 CFR Part 2 governs substance use disorder records, and it now sits much closer to HIPAA compliance enforcement than older mental models suggest. The 2024 final rule's compliance deadline was February 16, 2026.
The practical changes:
- Penalties: civil $25K to $1.5M per year; criminal $50K to $250K plus 1 to 10 years
- Consent: one consent can now cover treatment, payment, and healthcare operations together
- Privacy notice: a HIPAA-compliant Notice of Privacy Practices still needs additional Part 2 language for SUD records
State licensure adds the next layer. Therapy is legally located where the client is physically located at the time of the session. California, New York, and Illinois all require a full in-state license; PSYPACT extends to psychologists, while LMFTs, LCSWs, LMHCs, and LPCs rely on different compacts.
Multistate compacts shrink the timeline, but they don't erase credentialing work. PSYPACT, the Counseling Compact, the Social Work Compact, and IMLC all help in different lanes; a new state can still take 4 to 12 months.
If you're not HIPAA-covered, the FTC is your regulator
The FTC is the active regulator for apps outside HIPAA. Since 2023, BetterHelp, Cerebral, and Monument have all settled over health data moving into ad platforms or third-party tracking systems.
The pattern matters more than another round of dollar amounts. BetterHelp involved intake questionnaire data sent to Facebook, Snapchat, Pinterest, and Criteo. Cerebral's complaint named Google, Meta, TikTok, LinkedIn, and Snapchat pixels. Monument's named Meta Pixel events included "Paid: Weekly Therapy" and "Paid: Med Management," which made the event labels themselves part of the disclosure.
The FTC's view of patient data is broader than most builders expect:
- hashed emails
- IP addresses
- IMEI
- IDFA
- AAID
- Android ID
- Custom Audience names like "HIV" or "Birth Control"
Once a pixel carries that context to an ad platform, data security measures around the database stop mattering.
The behavioral-health-specific liability surfaces you inherit
Liability surfaces sit alongside HIPAA in the design conversation:
- DEA telehealth flexibilities extended through December 31, 2026 (fourth temporary extension). Schedule II-V remain prescribable via audio-video without a prior in-person visit. The Cerebral DOJ NPA is the cautionary tale for any app whose telehealth app development workflow includes algorithmic prescribing pressure.
- Duty to warn / Tarasoff exposure: when the app's risk model surfaces suicidality and a clinician on the platform sees it, whether the platform itself inherits the affirmative-warn duty is unsettled state by state.
- Mandatory reporting: child abuse, elder abuse, dependent adult abuse. The clinician files the legal report. Platform intake flow and risk-stratification logic decide whether reportable events ever reach that clinician.
These exposures get inherited even when the spec doesn't name them. Build the security measures that surface them to the right human at the right time.
Behavioral health EHRs don't look like Epic
The behavioral health EHR roster is Netsmart, Kipu, SimplePractice, TheraNest, Welligent, Alleva, and Sigmund AURA. Anyone creating a behavioral health app at scale plans EHR integration as a two-tier problem: two vendors with real developer experiences, five that require a sales conversation just to see a sandbox.
Two real integration targets, five "talk to sales" walls
The realistic-path column is the one to dwell on.
For most teams, the practical split is simple: build to Netsmart's CareConnect FHIR if the target customer is an enterprise behavioral health agency, and pay for Kipu's REST API to serve the addiction recovery vertical. The other five behavioral health software vendors require bespoke per-deal engineering or middleware.
Netsmart CareConnect is the only self-serve FHIR story
Netsmart's CareConnect is the closest thing behavioral health gets to a normal developer experience. The useful parts are specific:
- Standards: US Core 6.1.0, USCDI v1
- Auth: SMART on FHIR with OAuth 2.0
- Sandbox: public test environment at fhirtest.netsmartcloud.com
- Production path: self-serve app registration first, Netsmart sign-off before production
- Marketplace: launched April 15, 2024 with 50+ Partners, 3 Affiliates, and 170+ Members
If the target customer runs myAvatar, myEvolv, myUnity, or GEHRIMED, CareConnect is the first integration path to test.
Kipu is the paid REST API for addiction treatment
Kipu matters when the app serves addiction recovery: SUD residential, MAT, outpatient, or IOP. The path is a paid vendor relationship from day one.
Kipu's REST API has 41 endpoints, but only Patient supports write access. Everything else is read-only, which means treatment plans and clinical workflows need design around that constraint.
The access path is also slower than the API surface suggests. There's no public sandbox. Access is paid, requires a signed vendor agreement, and usually takes 3-5 business days plus 48 hours for activation.
Named integrations prove the path exists: Eleos Health in November 2023, Team Recovery in September 2025, then Kipu's acquisition of Team Recovery in April 2026.
Start the Kipu Circle conversation early. If write access matters to the workflow, finding out late is how a "simple integration" becomes a roadmap hostage situation.
For solo-practice marketplaces, EHR access is the bottleneck
SimplePractice has an Enterprise API, launched September 13, 2022 with KGA as the named customer, but access is gated to EAPs and managed care organizations. Solo practices and smaller healthcare providers usually can't get keys, so the integration path becomes middleware, custom workflow workarounds, or manual note transfer.
TheraNest and Welligent publish no API. Headway, Alma, and Grow Therapy run as parallel platforms; therapists who run one alongside SimplePractice still copy notes by hand.
For vendors that need FHIR to satisfy ONC (g)(10) Cures Act compliance without building it themselves, a shim pattern exists: Sigmund AURA contracted Darena Solutions / MeldRx in December 2022. Echo and EchoVantage, sister products under Ensora Health, the former Therapy Brands, publish Cures-Act-certified FHIR independently of Welligent.
The pattern: small-practice marketplaces are an integration dead end. Plan for manual export, scraping, or middleware, and price the deal accordingly.
How to build a behavioral health app in 7 steps
The traditional 7-step build path
Building a behavioral health app the traditional way runs seven phases across 9 to 18 months. The BH complications baked into each step are what most guides on how to create a behavioral health app skip entirely.
Step 1: Discovery (4-6 weeks)
Scope the app shape (D2C marketplace, EAP, clinical SaaS, peer support, PDT) and the regulatory exposure that comes with it. If the shape is clinical SaaS, CoCM economics get scoped here, including who can bill 99492-99494 and whether the psychiatric consultant model fits.
Step 2: Team assembly (6-12 weeks)
Recruit clinical informaticists, compliance-aware engineers, a HIPAA-trained designer, and (for SUD apps) someone who has read 42 CFR Part 2 cover to cover.
Step 3: UX/UI and clinical workflow design (8-12 weeks)
Screens that touch PHR cannot carry third-party tracking SDKs. The FTC pixel trap surfaces in audit later, when the marketing team has already shipped a campaign that depends on the events.
Step 4: Technical architecture (4-6 weeks)
Several BH-specific decisions get locked into the software development architecture here:
- 42 CFR Part 2 audit-grade access logging
- server-side analytics (no client-side trackers on PHR screens)
- crisis-pathway latency budgets
- PHR-grade encryption that survives FTC scrutiny
Step 5: Development sprints (4-6 months)
Validated instrument scoring (PHQ-9, GAD-7), crisis pathway integration, and EHR connectors (Netsmart or Kipu) eat the longest sprint cycles.
Step 6: QA + security + compliance (6-10 weeks)
HIPAA and 42 CFR Part 2 audit prep run in parallel with penetration testing and BAA chain documentation. Plan a separate review pass for any subprocessor that touches PHI or PHR.
Step 7: Multi-state credentialing and GTM (3-12 months overlapping)
Compact analysis (PSYPACT, Counseling Compact, Social Work Compact, IMLC) and per-state credentialing run concurrently with build, starting in week 1 if possible.
Total project timeline: 9 to 18 months from kickoff to ship. Three of the last five BH builds we audited overran by 4 to 6 months on Step 5 alone, almost always because of EHR sandbox timeouts.
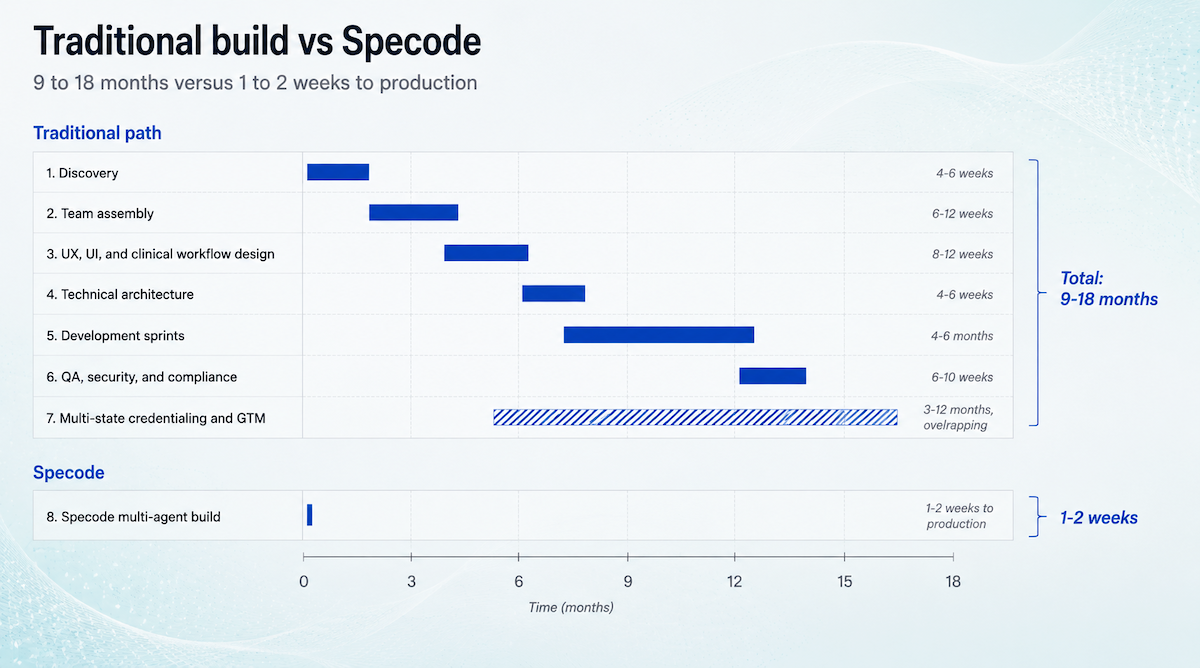
How Specode collapses this
Specode compresses the early build path into a guided, multi-agent workflow. The Planning agent scopes the app from a plain-English description, asking about shape, roles, data model, and v1 scope. The Design agent sets the system.
The Implementation agent can generate a working 3-5 screen build with role-based logins in roughly 10 minutes. That's the reviewable first pass. Focused builds can move into production review in 1-2 weeks instead of the 9-18 month traditional path. The HIPAA compliant foundation and backend hosting BAA come included on the Pro plan.
Generic tech stack advice fails in behavioral health
Generic stack advice gets healthcare app development most of the way to ship at the average tier: React Native, Node, Postgres, AWS, push notifications, done. Behavioral health mobile app development inherits a layer of constraints those generic recommendations skip. Each one earned its place in the behavioral health technology stack by being where a real app got hit.
Data layer
SUD records under 42 CFR Part 2 require audit-grade access logging with immutable trails:
- every read
- every write
- every export
- every deletion
Postgres alone won't do it. Plan a logging service (or RLS plus an audit table pattern) early.
PHR-grade encryption applies even when the user is not a HIPAA-covered patient: FTC-enforced cases treated hashed emails, IP addresses, IDFA/AAID, and Custom Audience names as identifiable health information.
Front-end and analytics
No third-party tracking SDKs on screens that touch PHR. Meta Pixel, Google Analytics SDKs on iOS and Android, Branch, AppsFlyer: every one of these has surfaced in an FTC complaint against a health app since 2023.
Analytics runs server-side or via privacy-preserving alternatives. Event names cannot contain health-status data; Monument's 'Paid: Weekly Therapy' event was itself the disclosure.
Crisis-pathway latency
The trigger-to-clinician-page path is measured in seconds. Notification stack reliability matters more than push notification UI polish. Twilio for SMS, OneSignal for push, and a dead-letter queue for the times when the primary channel fails are baseline.
Validated instrument scoring (PHQ-9, GAD-7, AUDIT, C-SSRS) lives in a server-side library (Python or Node) with versioned, audited scoring logic. Custom scoring on the client breaks the chain of custody when a clinician asks why the score was what it was.
The EHR section above points to the two connector paths most teams actually plan around: Netsmart FHIR for the agency vertical, and Kipu REST with HMAC auth for addiction recovery. Most BH stack failures we audit trace back to a single Meta Pixel that survived the production push.
Behavioral health has cost drivers general guides skip
Cost estimates for figuring out how to make a behavioral health app run wide because the spread depends on shape, integration scope, and clinician credentialing strategy. General healthcare app cost guides usually quote a $150K to $500K range. Behavioral health pushes the upper end higher because four cost lines get underweighted.
Multi-state clinician credentialing renews per state, per cycle
Plan on $1,500 to $5,000 per clinician per state for the initial license, plus renewal fees every cycle. Timelines still run 4 to 12 months in many states, even when compacts help.
The BH EHR integration premium is real money
Kipu's REST API requires paid access and a signed vendor agreement. Netsmart CareConnect marketplace fees scale by tier. FHIR-via-shim paths like Sigmund/MeldRx add their own licensing on top of build hours.
42 CFR Part 2 audit logging is its own line item
SUD records need immutable access trails:
- reads, writes, exports, deletions
- retention policies
- audit queries
- anomalous-access alerts
Implementing and operating that infrastructure is ongoing cost. Every audit cycle, every staff role change, every new state.
FTC-grade adtech hygiene costs more than people plan for
No third-party tracking on screens that touch PHR. Server-side analytics and custom event design replace the usual pixel setup, while every subprocessor adds legal review and BAA upkeep.
The reimbursement side changes the math too. Clinical SaaS apps in the CoCM lane can support around $145 per patient per month, billed by the primary care practice but enabled by the technology.
Hard dollar figures are deal-specific. Ranges help; fake precision doesn't.
How Specode helps you build a behavioral health app
Building a behavioral health app still needs clinical judgment, integration planning, and compliance review. Specode takes the scaffolding work off the blank canvas so teams shipping behavioral health solutions can spend their time on the parts only they can build.
- Plan before build. Specode's Planning, Design, and Implementation agents move in sequence, with approval before each handoff.
- Start from a HIPAA compliant foundation. Auth, data access patterns, audit-friendly workflows, and the Pro backend hosting BAA are built into the production path.
- Connect outside services on your terms. Specode can handle API-based integrations when users provide the required credentials, keys, and vendor access.
- Review before go-live. The HIPAA Compliance Agent scans code for potential issues by severity, and the Specode team reviews production apps before release.
- Keep the code. Export the source anytime, deploy elsewhere, and avoid rebuilding if the roadmap changes after Series A.
Preview links are for demos only and should never carry real PHI. For teams whose runway doesn't tolerate a 9-18 month build, Specode shortens behavioral health platform development to weeks without pretending the clinical complexity disappears.
What features actually move outcomes in a behavioral health app?
Validated measurement-based care (PHQ-9, GAD-7), real crisis pathway architecture, intentional clinician matching, and structured between-session work. Spring Health reports a 5.6-point PHQ-9 reduction and 1.9x ROI among frontline healthcare workers.
Frequently asked questions
No. The FTC is the active regulator for apps not covered by HIPAA. BetterHelp, Cerebral, and Monument settled for tracking-pixel violations between 2023 and 2024. 42 CFR Part 2 also applies to SUD records and runs stricter than HIPAA on consent.
Behavioral health covers the full psychiatric spectrum plus substance use disorder and addiction recovery. Mental health is the subset focused on mood and anxiety conditions, without the SUD records that trigger 42 CFR Part 2.
No. Licensed prescribers may use telehealth for Schedule II-V through December 31, 2026 without a prior in-person visit. AI itself cannot prescribe. Cerebral's DOJ NPA is the cautionary tale.
BH EHRs are a separate vendor ecosystem from Epic and Cerner. Two realistic developer targets exist: Netsmart's CareConnect FHIR for enterprise BH agencies, and Kipu's paid REST API for addiction treatment. The others require sales conversations.
Validated measurement-based care (PHQ-9, GAD-7), real crisis pathway architecture, intentional clinician matching, and structured between-session work. Spring Health reports a 5.6-point PHQ-9 reduction and 1.9x ROI among frontline healthcare workers.






