Addiction Assessment Tool Development: A Practical Playbook for Digital Screening Solutions

Addiction assessment tool development sounds straightforward on paper: take validated questionnaires, put them in an app, profit. Right? If only. Every founder and clinician who’s tried to digitize screening tools eventually hits the same wall: Why does something that looks like a simple form feel like launching a moon mission?
Because you’re not just building a form. You’re encoding trust, clinical rigor, and highly sensitive patient disclosures into a flow users won’t abandon after question three. You’re juggling psychometrics, regulatory expectations, integration headaches, and that one clinician who insists every question is “absolutely essential”—all while the CFO demands an ROI slide.
The truth: digital addiction assessments are powerful only when they’re designed, validated, and deployed with intention. This guide breaks down how to build them the right way—so your team can stop duct-taping surveys together and start delivering insights clinicians can rely on. Ready to save yourself six months of “How hard can it be?” conversations? Let’s go.
Key Takeaways
You don’t build trust in addiction recovery with shiny features — you earn it through clinical rigor, data integrity, and a deployment strategy that actually works in the field.
- Clinical credibility beats feature lists.
If your assessment logic isn’t backed by validated instruments (AUDIT, DAST-10, etc.) and doesn’t align with regulatory and payer expectations, you’re not building a medical product — you’re shipping a liability.
- Data architecture is where addiction-tech succeeds or fails.
Workflows must respect consent boundaries, multi-provider care, longitudinal tracking, and secure communication with external clinicians. The real differentiator is not UI — it’s compliant care pathways and data governance designed for addiction medicine.
- Reusable healthcare plumbing = faster validation, less risk.
Specode’s automated builder gives teams HIPAA-compatible components (auth, role-scoped data, secure messaging, clinical workflows) from day one, so founders can focus on the unique clinical model — not reinventing the same regulated infrastructure.
Understanding Addiction Assessment Tools
At a distance, addiction assessment tools look like glorified quizzes. Up close, they’re the front door to care for people dealing with substance abuse, substance use disorder, and co-occurring mental health issues. Which means they’re not just “nice UX” problems — they’re high-stakes decisions about who gets flagged, who gets missed, and what happens next.

In the context of addiction assessment tool development, you’re essentially building a translator between messy human stories and structured clinical assessment data. The tool has to capture nuance (shame, minimization, denial) while still outputting something a clinician, care coordinator, or payer can act on without a 40-minute chart review.
That’s a tough brief, especially when your stakeholders span founders, clinicians, and IT in overstretched behavioral health organizations.
Why Digital Addiction Assessment Matters Today
Digital tools aren’t just replacing clipboards; they’re changing when and where patient assessment happens:
- at intake
- in the waiting room
- via telehealth
- asynchronously at home
Done well, they reduce friction, standardize how risk is captured, and surface high-risk cases earlier instead of relying on whoever yells loudest in clinic.
From Paper Forms to Connected Clinical Assessment
The real shift is connectivity. Paper forms disappear into charts; digital assessments can push scores into EHRs, trigger alerts, and feed dashboards that actually influence staffing, outreach, and treatment planning. That’s the promise your product is being judged against, whether anyone says it out loud or not.
Where Assessment Fits in the Care Pathway
Screening is only step one. A modern tool has to support screening, diagnosis, and ongoing patient assessment — not just a one-time risk score that gets forgotten after the first visit.
Types of Digital Addiction Assessment Tools
When people picture a substance abuse assessment app, they usually imagine a mobile questionnaire. In reality, the landscape is much broader — and if you’re building a commercial product, knowing where you sit in that landscape determines everything from UX to monetization models.

Digital tools evolve around three main axes:
- who administers them
- where they’re completed
- how the data is used
Self-Administered vs Clinician-Guided
Self-administered workflows — whether via web or addiction assessment mobile app — lower the barrier for disclosure. Users can take their time, respond privately, and avoid the “fear of judgment” issue that derails honesty in clinic.
Clinician-guided assessments, on the other hand, allow real-time clarification and motivational interviewing tactics. If your product supports group therapy, intake visits, or telehealth sessions, this mode matters.
Most successful products support both: async intake + synchronous validation.
One-Time Screens vs Longitudinal Monitoring
A single standardized screen (e.g., AUDIT, DAST) gets someone into care. Longitudinal check-ins track whether treatment is actually working.
If your business model involves treatment centers or payer partnerships, recurring assessment is where the value lives — turn data into insights, insights into outcomes, outcomes into contracts.
Web Portals, Kiosks, Mobile, and Remote Models
- Mobile health flows are ideal for ongoing recovery programs
- In-clinic tablets reduce awkward conversations at the front desk
- Remote workflows support hybrid care and at-home honesty
The trend: tools that fit into life, not just into clinic workflows.
Evidence-Based Assessment Methods and Protocols
Digital assessments only work if they’re grounded in evidence-based assessment practices — otherwise they’re just dressed-up surveys. In addiction assessment app development, founders quickly learn that every question must map back to a validated framework, diagnostic criteria, or a recognized clinical decision point.

That’s the difference between a substance abuse evaluation tool a clinician trusts… and one they politely ignore.
Standardized Instruments and Diagnostic Criteria
The backbone of any assessment lies in established scales, for example:
- AUDIT
- DAST-10
- ASSIST
- CRAFFT (for youth)
These aren’t just checklists — they’re assessment protocols, statistical models distilled into questions. Each item influences severity scoring, risk assessment, and ultimately whether treatment should be escalated.
Digital tools also need to reflect clinical guidelines that evolve over time. Updating an instrument in software should be a configuration change — not a coding project that takes two sprints and a sacrificial developer soul.
Risk Assessment and Early Intervention Logic
Addiction care is a race against time. Tools that surface risk early enable early intervention strategies before someone becomes a crisis admission or a lost referral.
Modern flows use branching logic:
- High-risk answers trigger follow-up questions
- Scores may prompt clinician alerts
- Self-reported instability can auto-schedule outreach
That’s where digital surpasses paper: dynamic, adaptive questioning that feels human, not bureaucratic.
Codifying Evidence-Based Assessment into Flows
Clinical realism matters. You’re not just migrating a PDF — you’re redesigning how a conversation unfolds.
Work closely with addiction specialists to define:
- Which items require mandatory completion
- When to allow “I’d prefer not to answer”
- Which thresholds trigger emergency response rules
When workflows reflect real-world decision-making, the tool becomes a partner in care — not a compliance chore.
And yes, that means the software must respect nuance: patients minimize; clinicians probe; the app must support both truths simultaneously.
Key Features of Addiction Assessment Applications
If you stripped the logos off most tools in this space, you’d see the same thing: long forms, vague scores, and zero impact on decisions. To create addiction assessment application that stands out, you need features that make life easier for both patients and healthcare providers, not just your sales deck.

A User Interface That Encourages Radical Honesty
The user interface is not decoration here; it’s clinical infrastructure. If people feel rushed, judged, or confused, they lie or drop off.
Practical must-haves:
- Mobile-friendly flows that work on a cracked iPhone 8 in bad Wi-Fi
- Plain-language questions with just-in-time explanations
- Smart handling of “I’d rather not say” without breaking the scoring logic
If your addiction screening application doesn’t increase completion and honesty vs paper, it’s not a feature — it’s noise.
Structured Data Plus Real Clinical Decision Support
A good tool doesn’t just capture answers; it structures them into something a clinician can use in under 30 seconds. That’s where clinical decision support comes in.
Think:
- Clear severity bands (low / moderate / high risk)
- Flags for suicidality, polysubstance use, or co-occurring mental health red flags
- Smart suggestions for next steps in treatment planning
The output should feel less like a score report and more like a “what you should probably do next” nudge — without pretending to replace clinical judgment.
Features That Tie Directly to Patient Outcomes
The point of all this is better patient outcomes, not prettier dashboards. The platform should make it trivial to:
- Track changes in risk over time
- See which interventions follow which scores
- Give leadership a real view of how assessments translate into care
If you can show “we screened, we acted, things got better,” your assessment tool isn’t just software — it’s leverage in every conversation with payers, partners, and boards.
User Experience Design for Sensitive Assessments
Most people don’t open a behavioral addiction assessment tool thinking, “Can’t wait to share my worst decisions with a web form today.” If your UX ignores that basic truth, completion rates plummet and your beautifully modeled scoring logic becomes analytics theatre.

Designing a Tool Patients Actually Complete
For users, this isn’t “onboarding”; it’s emotional risk. Good UX lowers that perceived risk: short segments, clear progress, soft landings after tough questions, and the option to pause without losing everything.
Think in episodes, not endless scroll: 3–5 questions per screen, with clear signals about why this matters for addiction treatment (“This helps your clinician choose the safest next step”), not just “required fields.”
Micro-wins (“You’re almost done” when they’re genuinely almost done) are more powerful here than fancy animations.
Stigma, Trust, and Microcopy for Difficult Questions
The copy is doing clinical work. Questions about relapse, overdose, or high-risk use need context:
- Normalizing statements (“Many people in addiction recovery experience this…”)
- Safety framing (“Your answers help us choose the right level of support.”)
- Honest boundaries (“Your responses may be reviewed by your care team.”)
If a question would feel harsh read aloud in a session, it’s probably worse on a screen. Build with clinicians who are used to motivational interviewing, not just product people who are good at signup funnels.
Accessibility, Language, and Cultural Considerations
If your tool only works for highly literate, neurotypical users on fast Wi-Fi, it’s not ready for real-world rehabilitation facilities.
Non-negotiables:
- Plain language, no DSM-speak in the UI
- Support for different reading levels and languages
- Mobile-first flows that tolerate bad connections and older devices
The UX bar here isn’t “delightful.” It’s “safe enough that people tell the truth when it’s hardest to.”
Technology Stack for Assessment Tool Development
In addiction evaluation software development, your tech stack is basically a list of ways you can either help or sabotage clinicians at scale. The goal isn’t to chase every shiny framework; it’s to pick tools that are boringly reliable under real clinic load, easy to evolve, and friendly to regulated environments.

Core Architecture for Web and Mobile Frontends
Start by assuming multi-channel from day one: responsive web + mobile-friendly flows at minimum. Frontends should handle offline-tolerant questionnaires, secure session handling, and smooth transitions between “quick screen” and “deeper assessment” modes.
Reuse as much UI logic as possible so a change to a question, hint, or score description doesn’t turn into a four-client regression party.
Back-End Services, Databases, and Messaging
The back end has three jobs: store sensitive data safely, orchestrate assessment logic, and send the right signals to clinicians and systems (alerts, tasks, follow-ups). You’ll want a relational database for traceability, strong audit logging, and a service layer that can:
- Version assessment instruments cleanly
- Separate PHI from analytics views
- Support async notifications without duct-taped cron jobs
This is also where you lay the foundation for serious data analytics later instead of scraping CSVs in panic right before a payer meeting.
Where Mental Health App Patterns Still Apply
A lot of what works in mental health app development carries over here: role-based access, consent flows, secure messaging, symptom tracking, and outcome measurement. The difference is that in an assessment-heavy digital therapeutics context, the stack has to treat questionnaires and scoring rules as first-class objects — not hardcoded forms.
Architect for “swap out this instrument” and “add a new protocol” as configuration, not a rewrite. Future you (and your clinicians) will be grateful.
Clinical Validation and Testing Requirements
Here’s the part founders often underestimate. In substance abuse screening tool development, shipping the software is only halftime. The other half is proving that your digital instrument actually measures what it claims — consistently, accurately, and in real-world messy contexts. Otherwise, clinicians will treat your tool like a horoscope with better typography.

Designing Studies for Substance Abuse Screening Tool Development
Paper-based instruments earned trust through research:
- controlled studies
- large sample sizes
- peer-reviewed evidence
When digitized, those assumptions can break. Fonts, ordering of items, screen size, even whether a question wraps to a new line — all can alter responses.
You’ll need clinical validation in environments that reflect where your tool will live: intake rooms, telehealth sessions, emergency departments, halfway houses. And the sample should include the population your clients actually serve — not just “easy-to-recruit college students who like gift cards.”
Psychometric Properties in a Digital Context
The gold standards still apply:
- Validity testing — do scores predict risk and severity correctly?
- Reliability testing — do repeated screens yield consistent results when nothing has changed?
- Test–retest intervals — long enough to avoid memory effects, short enough to avoid real clinical change
And don’t forget digital-specific risks: “select-all-that-apply” fatigue, accidental taps, and people scrolling past nuance because the bus just hit a pothole.
From Pilot to Rollout: Iterating with Real Clinics
Start small: one site, one workflow, one cohort. Observe everything. Did staff bypass it because it added friction? Did patients skip optional questions that shouldn’t have been optional? Did scoring delay care?
Once validated, expand gradually, keeping a rapid feedback loop open with clinicians who don’t sugarcoat things. This isn’t just QA — it’s part of clinical proof.
Digital tools win when the data proves the tool improved triage, sped access to care, or prevented bad outcomes. That’s the story every buyer wants to hear — and clinical testing gives you the receipts.
Integration with Treatment Management Systems
A standalone assessment is basically an expensive clipboard. In addiction screening software development, the real value emerges when scores trigger action — tasks, referrals, outreach, care changes — inside systems clinicians already live in.
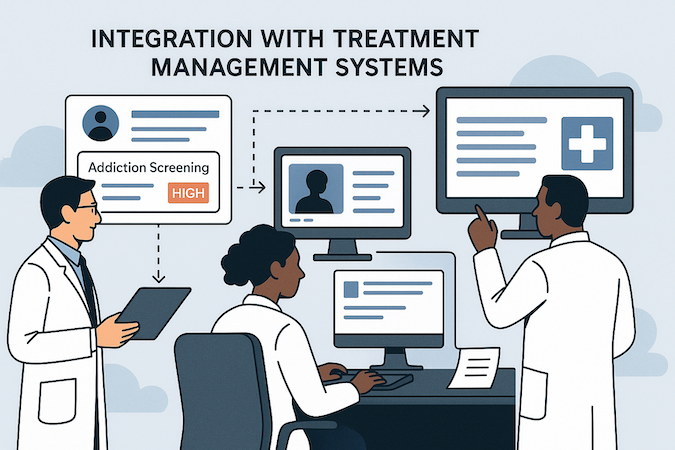
Embedding Assessments into Existing Treatment Workflows
The prime directive: don’t create parallel workflows. If a clinician must log into “yet another platform” just to see the result, that result is already stale.
Integration points worth prioritizing:
- Intake → attach screen results to patient profile before the first session
- Inpatient/IOP → trigger monitoring schedules based on severity
- Discharge → update risk level to shape recovery support
Every touchpoint should feel native to the experience provider teams already trust.
Telehealth Integration and Session Prep
Telehealth isn’t just video — it’s a planning engine. With telemedicine app development features built-in, assessments can:
- Auto-send screens before virtual appointments
- Prioritize urgent cases in the telehealth queue
- Feed talking points into the clinician’s prep window
This prevents awkward “So why are you here today?” calls and turns remote care into proactive intervention.
Syncing Results with EHRs and Case Management Tools
If results don’t land in the electronic health records system, they don’t count from a billing, compliance, or continuity-of-care perspective.
Minimum viable EHR integration checklist:
- Standardized data packets (FHIR where possible)
- Role-based visibility of sensitive details
- Clear audit trails for who accessed what and when
Clinicians want fewer tabs, not another analytics island. Integrations make your tool part of their clinical heartbeat — not an occasional extra.
Data Security and Privacy Considerations
In digital addiction assessment development, you’re dealing with some of the most sensitive PHI imaginable — details many people haven’t even told their closest friends. If your product doesn’t feel safe, users will censor themselves. If it truly isn’t safe, regulators will eventually censor you.
Handling PHI Safely in Digital Addiction Assessment Development
This isn’t a feature — it’s the foundation. Encryption in transit and at rest is table stakes; the real differentiators are:
- Strong authentication with minimal friction
- Fine-grained access controls (no “everyone on the care team sees everything”)
- Context-aware alerts for high-risk disclosures (but only to the right people)
Never store what you don’t absolutely need. Therapy-grade trust requires ruthless data minimization.
Data Minimization, Retention, and Access Controls
A clean data model answers:
- What PHI do we store?
- Why?
- For how long?
- Who can see it? And under what circumstances?
If answers to those questions involve guesswork, you’re courting risk. Good data privacy practice means letting patients revoke consent, delete accounts without Kafka journeys, and receive clear explanations about how their information is used to support their care.
Audit Trails, Logging, and Incident Response
People in addiction assessment tool development often treat audit logs like a dull checkbox — until something goes wrong. Then logs become the only thing between you and a compliance meltdown.
Essentials:
- Immutable logs tracking every access/edit
- Role-based filtering (security sees everything; frontline staff see only what’s relevant)
- A rehearsed incident-response plan — not “we’ll draft one after the breach”
You don’t need a paranoia culture. You do need a culture where privacy is invisible because it’s engineered into every click.
Regulatory Compliance for Addiction Assessment Tools
“We’ll worry about compliance later” is how promising products become un-purchasable prototypes. When you develop addiction screening tool solutions, you’re entering one of the most regulated corners of healthcare — and the rules shift depending on where the tool sits in the care workflow.
Regulatory Landscape for Substance Use and Mental Health Tools
The baseline guardrails:
- Privacy regulations (HIPAA compliance in the U.S., GDPR in Europe)
- Clinical practice guidance for substance use assessments
- State-specific substance use data laws (some of the strictest in healthcare)
But depending on features, classifications may change fast:
- Does your tool guide diagnosis?
- Provide treatment recommendations?
- Influence clinical decisions that affect safety?
The more clinical control the software assumes, the closer it moves toward medical device classification — with the scrutiny that comes with it.
Aligning Digital Flows with Clinical and Payer Expectations
Major buyers — health systems, provider groups, payers — have checklists. And compliance is just one column. They’ll ask:
- Is this workflow evidence-aligned?
- Does it produce usable documentation for care coordination?
- Can results support reimbursable care steps?
If you can tie assessment output to recognized decision pathways, you’ll unlock purchasing, adoption, and reimbursement much faster.
Documentation and Evidence for Approvals and Partnerships
Compliance isn’t vibes — it’s paperwork. Be ready to provide:
- Methodology for instrument digitization
- Scoring logic transparency
- Policies for consent, privacy, and clinical escalation
- Clinical evaluation results
- Governance records for updates and corrections
When procurement teams ask for validation proof and you can send a clean folder instead of a panic Slack chain — that’s when you know you’re enterprise-ready.
Machine Learning and Predictive Analytics Integration
ML sounds like magic until clinicians ask, “So what exactly is the model doing?” Adding intelligence to substance use assessment tool creation can be transformative — or terrifying — depending on how transparent and clinically appropriate it is. This is where hype has to take a back seat to trust.

Use Cases Where ML Actually Helps
If your machine learning claim is “better insights,” that’s marketing. If it’s driving a decision worth taking seriously, then we’re talking:
- Identifying relapse risk patterns earlier than provider intuition
- Predicting engagement drop-offs to trigger outreach
- Highlighting co-occurring mental health concerns that often hide in plain sight
ML shines in pattern recognition, not replacing validated clinical scoring. Treat it as augmentation, not automation.
Predictive Modeling for Relapse and Severity Scores
Severity snapshots are useful — trendlines are life-saving. Predictive modeling can contextualize scores over time:
- What’s this patient’s risk tomorrow given recent changes?
- Which triggers correlate with future clinical deterioration?
- When should the care team intervene before a crisis?
The trick is grounding your model in clinically meaningful features: recent disclosures, attendance patterns, sudden mood shifts… not irrelevant digital breadcrumbs like screen tap velocity.
Guardrails: Bias, Interpretability, and Clinician Trust
If a model pushes a red flag and the clinician can’t explain why, adoption collapses. Guardrails to bake in from day one:
- Bias audits across demographic groups
- Clear attribution for what influenced the prediction
- Conservative thresholds with human-in-the-loop overrides
AI needs humility: clinicians must stay in charge, and patients must never feel judged by an opaque algorithm.
Development Process: From Concept to Deployment
The biggest lie in health tech is “we’ll refine the workflow after launch.” In reality, the way you build addiction screening platform workflows in the early stages pretty much locks in your clinical, technical, and business constraints for years. So you might as well get intentional about the process.
Discovery: Clinical Requirements, Stakeholders, and Constraints
Discovery is where you decide whether you’re building a serious clinical tool or a fancy survey. The difference is who’s in the room. You don’t want just “someone from the clinic”; you want the people who actually feel the pain:
- Clinicians who do assessments daily
- Intake staff who see where patients get stuck
- Program directors who own outcomes and compliance
- A technical lead who can say “that’s a three-month ask” before it’s printed in a brochure
Key outcomes from discovery:
- Clear definition of the target population and use cases
- Agreed list of instruments and decision points (not 15 “maybe someday” screens)
- Constraints around integration, devices, staffing, and regulatory requirements
If you can’t summarize the product in a single “job to be done” for each stakeholder, you’re not ready to spec features.
Prototyping, MVP, and Iterative Co-Design with Clinicians
Your first clickable flow is not for investors — it’s for the crankiest clinician you can find. If they’ll use it, everyone else will.
Patterns that work:
- Low-fidelity first: clickable wireframes to debate content and flow, not pixel-perfect color choices
- MVP scope: one core pathway end to end (e.g., alcohol screening → risk stratification → suggested next steps)
- Co-design cycles: short feedback loops where clinicians see their input reflected quickly
Think in “thin slices”:
- One cohort (e.g., outpatient adults)
- One channel (e.g., in-clinic tablet)
- One primary journey (e.g., intake)
Ship that, validate it, then expand. MVP is not a demo that “kind of works.” It’s one workflow that really works in the wild.
Go-Live, Monitoring, and Continuous Improvement Loops
Deployment isn’t an event; it’s a series of experiments with higher and higher stakes. A decent go-live plan includes:
- Staff training that shows “what changes on Monday,” not 40 slides of architecture
- A support channel where front-line teams can complain without politics
- Clear success metrics (completion rates, time-to-screen, high-risk detection, no-show reduction, etc.)
Post-launch, treat the platform like a living protocol:
- Review analytics weekly at first, then monthly
- Capture edge cases and “workarounds” staff invent
- Schedule regular clinical governance reviews for instrument and logic updates
The goal isn’t to prevent every change after go-live. It’s to make change safe, traceable, and fast — so the tool stays aligned with how care is actually delivered, not how it looked in last year’s slide deck.
Cost Factors in Addiction Assessment Tool Development
Building an addiction recovery assessment app isn’t a fixed-price Fiverr gig. Depending on scope, integration, compliance, and ambition, you could be looking at anything from a modest prototype to a near-enterprise platform.
What Recent Benchmarks Say
- According to a 2025 breakdown, a basic healthcare/mobile health app (minimal features, no heavy integrations) can start around US $50,000–$100,000.
- Medium-complexity apps — e.g., with a few integrations, moderate UI/UX and some backend logic — typically land in the US $100,000–$250,000 band.
- For full-featured, compliance-heavy, multi-role (patient, clinician, admin) apps — especially those integrating with EHRs, telehealth modules, audit/logging, and secure data storage — costs commonly climb toward US $250,000–$450,000+.
- And maintenance isn’t trivial: ongoing support, security patches, updates and compliance upkeep often require 15–25% of the original development cost per year.
These are industry-wide numbers — for a behavioral-health assessment app, expect the high end (or more) when you account for privacy, validation, and EHR integrations.
Scope, Integrations, and Clinical Complexity as Cost Drivers
Where you sit in that spectrum depends critically on three intertwined levers:
Scope
- A minimal “intake questionnaire → risk score” flow might stay near the lower end ($50–100K).
- Add longitudinal monitoring, multiple validated instruments, branching logic, clinician dashboards, and outcome tracking — and you’ll ratchet cost substantially upward.
Integrations
- No external systems (stand-alone): cheaper and faster.
- Basic integrations (export to CSV, read-only EHR export): moderate cost bump.
- Deep integrations (bi-directional EHR sync, telehealth hooks, role-based clinician portals, secure audit logging): these push you into the $250K+ range — often a deciding factor between a pilot and enterprise-grade launch.
Clinical Complexity
- Static screening thresholds is easiest.
- But if you support multiple instruments (e.g. alcohol, opioids, behavioral addictions) — each with validation needs — and wish for branching logic, role-specific outputs, and real-time alerts, the complexity (and certifiable QA, compliance, validation) becomes a major cost driver.
In short: every “nice-to-have” becomes a real line item when you quote engineering, testing, compliance, and QA.
Comparing Custom Builds, Off-the-Shelf, and Platform-Based Approaches
* These ranges are drawn from recent industry data for healthcare apps; actual cost for an addiction recovery assessment app will skew toward the higher end due to complexity, compliance, and potential integrations.
Reality Check: Cheapest ≠ Smartest
If you just want a survey app for internal use — go off-the-shelf or DIY. But if you aim for enterprise-grade adoption (clinics, rehabilitation facilities, payers), treating security, privacy, validation, and integrations as “nice to have” will sink you.
The “cheapest” credible tool is often the one that gets to real-world usage and validated outcomes fastest — not the one with the lowest sticker price.
Monetization Models for Assessment Platforms
There’s no single “right” way to monetize addiction assessment tool development — but there are definitely wrong ones. Selling to individuals rarely works (no one Googles “I might have a drug problem” and then buys a subscription).
The money flows where the care is delivered: treatment providers, payers, and health systems who need assessments to drive better outcomes and reimbursement.
B2B SaaS for Treatment Centers and Health Systems
The most common path:
- Per-provider or per-clinic licenses
- Tiered pricing by number of assessments/month
- Enterprise features (dashboards, integrations) reserved for higher tiers
This aligns value (better triage + throughput) with revenue and makes procurement happy because it maps to operational budgets.
Licensing, White-Label, and Revenue-Share Models
Some organizations want your product… but with their branding and workflows. White-label + licensing lets them feel ownership while you keep the IP. Revenue-share is growing in residential and outpatient addiction treatment segments — especially where improved outcomes can unlock reimbursement uplifts. Risk-sharing makes buyers say yes faster.
Bundling Assessments with Broader Digital Therapeutics Offerings
Standalone assessments have a ceiling. When bundled with:
- Remote support
- CBT-based interventions
- Care-team messaging
- Outcome tracking linked to payer value metrics
…screens become an engine driving engagement and justification for long-term contracts (think digital therapeutics meets “evidence of benefit” reporting).
Assessments are rarely the product by themselves — they’re the trust mechanism that gets you into the clinical workflow and keeps you there as you expand your footprint.
How Specode Helps Develop Addiction Assessment Apps
Writing an addiction recovery app development guide is one thing. Shipping a production-grade clinical product is a completely different sport. And most founders discover that the expensive part of “building software” isn’t actually the software — it’s the healthcare plumbing: HIPAA, roles/permissions, audit logs, secure messaging, scheduling, outcomes tracking, and yes… every integration a clinician could dream up.
Specode exists so you don’t have to reinvent all that from scratch.

Instead of handing you a blank canvas, Specode starts you with a functioning, HIPAA-ready healthcare foundation — patient, provider, and admin portals already wired together — then lets you shape it into your clinical workflow.
Inside the platform you get:
- Reusable HIPAA-compliant components, pre-built for behavioral health and clinical intake
- AI-assisted assembly using natural language — describe what you want, Specode builds and wires the components
- Code ownership, so you can keep scaling without platform lock-in
- Ready-to-integrate telehealth, scheduling, basic EMR, secure chat — all designed for remote assessment workflows out of the gate
This isn’t a “no-code toy” — it’s an acceleration lane built by a team that has delivered real, regulated healthcare products for years. When needed, Specode’s engineers step in to customize things like EHR connectivity, advanced role logic, and outcome dashboards — without hijacking your roadmap.
And we have proof. Teams building far more complex solutions than a screening tool have launched 7-figure ARR products in months — not years — using Specode as their backbone.
Whether you’re building a simple intake triage or a full continuum of care platform, Specode gives you a faster path through every stage of addiction assessment app development — from prototype to pilot to enterprise-ready deployment.
Let’s assemble the backbone of your clinical workflow — and make your V1 the one that actually goes live.
Frequently asked questions
Most digital tools start with a small, well-known core: instruments like AUDIT/AUDIT-C (alcohol), DAST-10 (drugs), and ASSIST (multi-substance). For youth, CRAFFT is common. On top of that, many teams add brief depression/anxiety scales (e.g., PHQ-9, GAD-7) because co-occurring mental health issues are the rule, not the exception. The key is to pick a minimal set that your clinicians will actually use and that map cleanly into risk bands and next-step recommendations.
Start from validated paper instruments, preserve question wording and scoring rules, and then run digital-specific validation: pilot in real clinics, compare digital scores to clinician judgment and outcomes, and perform reliability and validity testing (e.g., test–retest, internal consistency, correlation with known measures). Treat this as a structured clinical validation phase, not “UAT with nicer coffee".
In the U.S., you’re usually dealing with HIPAA, plus potentially stricter state laws for substance use data. In other regions you’ll encounter GDPR or equivalent privacy frameworks. Practically, that means PHI-safe hosting, encryption, access controls, consent flows, and clear policies for retention, breach handling, and patient rights (access, correction, deletion where applicable).
AI is best used as augmentation: spotting patterns across many patients (e.g., relapse risk trends, engagement drop-offs) and proposing risk flags or next steps that clinicians can review. It should not replace validated instruments or human judgment. Good implementations use transparent features, conservative thresholds, and always keep a clinician in the loop.
A focused MVP (one core flow, limited integrations) might take a few months to design, build, and pilot. A full platform with multiple instruments, deep integrations, and rigorous validation usually runs closer to 6–12 months. Using a healthcare-focused platform like Specode can compress the “plumbing” timeline significantly, so more of that time goes into clinical design and real-world testing instead of boilerplate.





