Second Opinion Platform Development: A Complete Guide for Healthcare Founders

Every year, an estimated 12 million Americans receive the wrong diagnosis — roughly 1 in 20 adults — and approximately 795,000 die or suffer permanent disability as a result of misdiagnosis (Newman-Toker et al., BMJ Quality & Safety).
For teams evaluating second opinion platform development, the clinical case is compelling.
A Mayo Clinic study found that only 12% of referred patients had their original diagnosis fully confirmed; 21% received a completely different diagnosis, and 66% had theirs meaningfully refined. Cleveland Clinic's virtual second opinion program reports a 28% diagnosis change rate. Accolade reports 35% of consults lead to an alternate diagnosis altogether.
Despite clear evidence that second opinions improve diagnostic accuracy and reshape the treatment plan review process, most patients never seek one. The barriers are familiar: access, cost, and friction. That gap between clinical evidence and patient behavior represents a significant — and largely unmet — product opportunity.
How do you build a medical second opinion platform?
A medical second opinion platform requires three core layers: a patient-facing case submission and records upload system, a provider-facing review workflow with DICOM imaging support and structured opinion templates, and an admin layer handling case routing, credentialing, and audit logging. The entire stack must be HIPAA-compliant with BAAs across every vendor. Most teams choose async (store-and-forward) as the default consultation model, with optional live video escalation. Expect 12–18 months and $400K–$1M+ for a custom build, or 6–12 weeks using an AI-powered healthcare app builder like Specode.
Key Takeaways
- Async-first is the dominant architecture. Complex diagnostic cases — oncology, pathology, radiology — benefit from deep specialist review, not 30-minute video calls. Build async as the default, sync as the escalation path.
- Records ingestion is the hardest technical problem. Patients don't have their records in one place. Plan your approach early — patient self-upload, FHIR/HL7 EHR integration, or retrieval services like Particle Health and Datavant — because this decision shapes your entire data architecture.
- Compliance is structural, not cosmetic. PHI accumulates across every layer of a second opinion platform — records, imaging, clinical notes, specialist opinions. BAA coverage, audit logging, role-based access, and cross-state licensing need to be designed in from day one, not bolted on before launch.
What Is a Medical Second Opinion Platform?
A medical second opinion platform connects patients — or their referring providers — with specialist reviewers for independent clinical review of a diagnosis or treatment plan. These platforms handle teleconsultation through asynchronous consultation (records submitted and reviewed offline) or live video, managing the care coordination layer between the patient, their existing provider, and the reviewing specialist.
This is distinct from primary telehealth services like Teladoc or MDLive, which focus on virtual urgent or primary care, and from provider-to-provider eConsult tools used internally within health systems. Second opinion platforms sit in between: they route complex cases to subspecialists for deep diagnostic review.
A few established players illustrate the model.
- Cleveland Clinic's MyConsult (delivered via its Amwell joint venture) covers 1,200+ diagnoses across 550+ subspecialties.
- Transcarent — which acquired Accolade for $621M in 2025 — operates the 2nd.MD expert opinion service across 20M+ members.
- Included Health offers its Expert Medical Opinion service to employers.
All operate within healthcare compliance frameworks, though with meaningfully different architectures under the hood.
Market Opportunity & Who's Building This
The global market for digital second opinion services is valued in the mid-single-digit billions and projected to more than double by 2030, with CAGRs ranging 12–16% depending on the source.
North America accounts for roughly three-fourths of that market. Oncology second opinion is the largest segment; cardiology is the fastest-growing. Key drivers include:
- rising diagnostic complexity
- expanding insurance coverage
- employer cost-optimization (health plans save an estimated $5K–$8.7K per consultation)
- sustained telemedicine adoption post-pandemic
The builders fall into four camps:
- Health systems adding a revenue cycle line — Cleveland Clinic, Yale Medicine, Stanford Medicine, and New York-Presbyterian all now run virtual second opinion programs.
- Employer benefit platforms operating subscription model or marketplace model pricing — Transcarent/Accolade/2nd.MD and Included Health.
- Specialty-specific startups like Cancer Expert Now, focused purely on oncology.
- AI-assisted pathology companies like PathAI and Paige — not patient-facing platforms themselves, but diagnostic infrastructure that makes specialist review faster and more accurate.
Types of Second Opinion Platforms
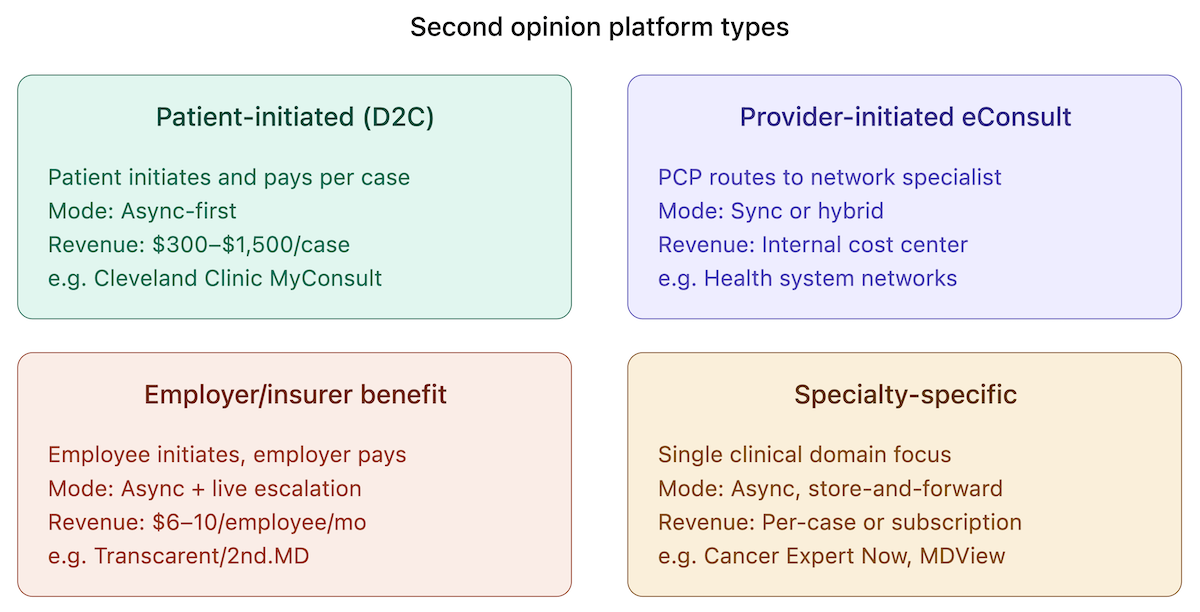
Not all second opinion telemedicine platforms work the same way. The model you build depends on who initiates the review, who pays, and how cases flow through the system. Four distinct types have emerged, each with different workflow, compliance, and monetization implications.
Patient-Initiated (D2C)
Patients upload records through a patient portal and pay per case. Cleveland Clinic's MyConsult is the clearest example — $565 per case, $745 with pathology review. These tend to be async-first, since complex cases benefit from deep specialist review rather than a live call.
Provider-Initiated eConsult
A PCP uses case routing to refer a patient to a specialist within a provider-to-provider network. The patient may never interact with the platform directly. These skew synchronous or hybrid depending on the health system's internal workflow.
Employer/Insurer Benefit
Second opinions embedded as a covered benefit — Transcarent/2nd.MD and Included Health's Expert Medical Opinion both operate this way, with the employer paying a per-employee fee. Predominantly async with optional live escalation.
Specialty-Specific
Platforms built for a single clinical domain — Cancer Expert Now for oncology, MDView for radiology second opinion. PathAI and Paige serve as AI-assisted diagnostic layers within pathology workflows rather than patient-facing tools. These tend toward async, store-and-forward models suited to imaging-heavy review.
Core Features of a Second Opinion Platform
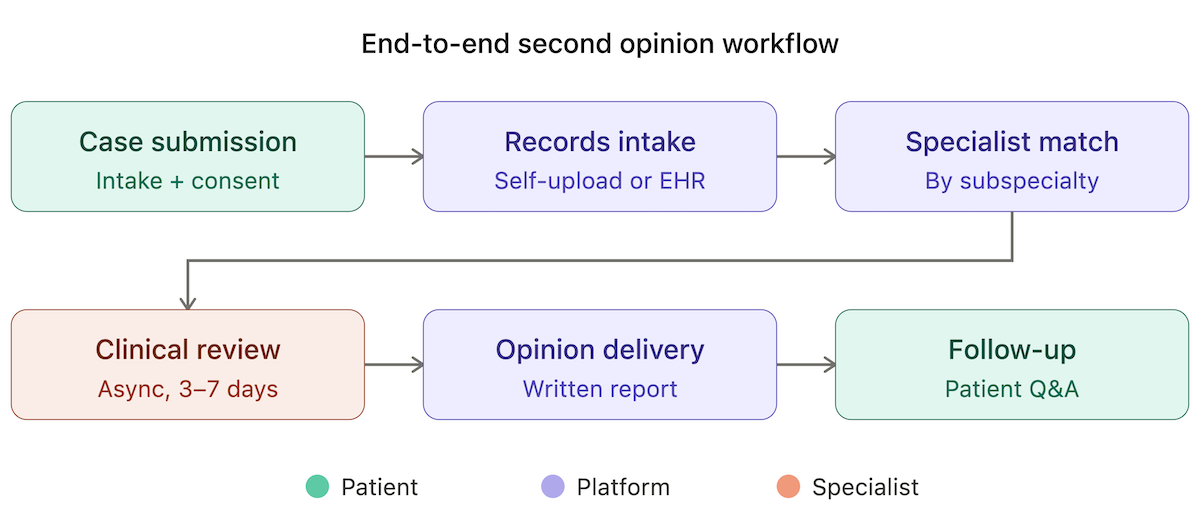
To build a second opinion app, you need three layers of functionality: patient-facing, provider-facing, and admin/ops.
Patient-Facing
- Case submission workflow with structured intake forms
- Medical records upload supporting PDFs, lab results, and DICOM imaging files
- Patient consent management capturing patient authorization for record release and specialist review
- Case status tracking so patients can follow their case through each stage
- Secure file transfer for sensitive documents
- Opinion delivery — typically a written report with findings and recommendations
- Follow-up Q&A allowing patients to ask clarifying questions after receiving the opinion
Provider-Facing
- Case queue with filtering by specialty, urgency, and turnaround time
- Integrated records viewer with DICOM support for reviewing imaging inline
- Structured opinion templates standardizing how specialists document findings
- Turnaround time and SLA management — dashboards and alerts ensuring cases hit committed windows
- Billing integration connecting completed cases to payment or reimbursement workflows
Admin/Ops
- Provider credentialing tracking
- Case routing and matching logic assigning incoming cases to the right specialist
- Quality assurance workflows — peer review flags, completion audits, patient satisfaction scoring
- Audit logs recording every action on a case, from record access to opinion submission
The specifics of how records flow into the platform, how credentialing works, and what compliance architecture underpins all of this are covered in dedicated sections below. At this stage, the goal is simply mapping the surface area of what you're building.
The Async vs. Synchronous Consultation Decision
This is a foundational product architecture decision for any online second opinion platform, and it shapes everything downstream — scheduling infrastructure, specialist compensation, scalability, and the type of cases you can handle well.
Asynchronous (Store-and-Forward)
The patient submits records; a specialist reviews them independently and returns a written opinion. No scheduling, no time-zone constraints, no live coordination overhead. This model suits complex diagnostic cases — oncology, pathology, radiology — where the specialist needs hours of focused review rather than a 30-minute conversation. It scales better because specialist time isn't locked to a calendar slot.
Cleveland Clinic's MyConsult is primarily async: the specialist reviews uploaded records, prepares a written report, and offers an optional virtual visit follow-up. Opinions are delivered within 3–5 days. This is the dominant model among asynchronous telemedicine platforms built for deep diagnostic review.
Synchronous (Live Video/Phone)
The patient speaks directly with a specialist in real time. Higher-touch, better for cases that need dialogue — situations where the specialist wants to ask follow-up questions, perform a visual assessment, or walk a patient through a complex treatment decision. The tradeoff is that it's harder to scale. Every case requires a scheduled block of specialist time.
2nd.MD (now Transcarent) uses this model: patients consult specialists by phone or video, typically within 3–5 days of case submission.
Where Most Platforms Land
Most mature specialist consultation platforms default to async with sync as an optional escalation path. This gives you the scalability of store-and-forward for the majority of cases while preserving the option for live dialogue when a case warrants it — a practical starting point for any telehealth app development team building in this space.
HIPAA & Compliance Architecture
Second opinion software development carries heavier HIPAA compliance requirements than most telehealth builds. The reason is data surface area: PHI doesn't just pass through the platform — it accumulates. Medical records, imaging studies, pathology reports, and clinical notes all flow in from multiple sources, get reviewed by specialists who may sit outside the originating health system, and persist as part of the case record. Every touchpoint is a potential exposure point. Building a truly HIPAA compliant second opinion service means addressing all of them.
The baseline requirements:
- BAA coverage across the entire vendor stack. Every service that touches PHI — cloud infrastructure, messaging, file storage, video, analytics — needs a signed HIPAA Business Associate Agreement. No exceptions, no "we'll add it later."
- Consent capture for record release. Patients must authorize the transfer of their records to the platform and to the reviewing specialist. This needs to be auditable, timestamped, and specific to each case.
- Audit logging of every record access. Who viewed what, when, and from where — across patient, provider, and admin roles. This isn't optional; it's a HIPAA requirement and a liability shield.
- Role-based access controls. Reviewers see only their assigned cases. Admins manage workflows but may not need access to clinical content. Patients see their own records and the final opinion. Each role gets the minimum necessary access.
Cross-State Licensing: The Overlooked Compliance Layer
Second opinion platforms frequently route cases across state lines, which means the reviewing specialist must be licensed in the patient's state.
The Interstate Medical Licensure Compact (IMLC) streamlines this — 41 states plus DC and Guam now participate, with over 152,000 license requests processed since 2017 — but it's an expedited pathway to obtain separate state licenses, not a single multistate license.
California, Florida, and New York remain notable non-participants. Beyond licensure, malpractice coverage across state lines presents an additional barrier flagged at ATA EDGE 2025. For clinical decision support platforms routing cases nationally, this compliance layer needs to be designed in from day one.
EHR Integration & Medical Records Handling
This is the hardest technical layer in any medical second opinion app. Patients rarely have their records in a single place, and getting those records into your platform reliably is the first engineering challenge you'll face. There are three pathways, each with different tradeoffs for EHR integration.
Patient Self-Upload
The simplest approach: patients upload PDFs, lab reports, and DICOM imaging files directly. Low integration cost, but it puts the burden entirely on the patient — and most patients don't have clean, complete copies of their own records.
EHR Integration via FHIR/HL7
Direct connection to health system EHRs using FHIR and HL7 standards. This is the most scalable path to true EHR interoperability, but also the hardest to implement — each health system has its own EHR configuration, consent workflows, and data formats. Plan for long integration timelines per partner.
Medical Records Retrieval Services
The middle path. Particle Health provides API access to 320M+ patient records from 70,000+ healthcare organizations — single API, FHIR-formatted output, BAA included, with AI-powered summarization through its Insights Platform. Datavant is the largest retrieval company in the US, pulling 64M+ records annually from 80,000+ hospitals and clinics. Various smaller regional services also exist.
Medical Imaging (DICOM)
Medical imaging requires its own stack. For viewing, OHIF Viewer (currently v3.11) is the leading open-source, zero-footprint, web-based option — built on the Cornerstone3D rendering library and the basis for many FDA-cleared clinical viewers. For storage, Google Cloud Healthcare API offers managed DICOMweb-compliant DICOM storage with built-in de-identification and BigQuery export; AWS HealthImaging provides a comparable managed option. Self-hosted alternatives like Orthanc and dcm4chee remain viable for teams that need full control.
Provider Network & Credentialing
The platform is only as good as its specialist network. Building, vetting, and managing the supply side is an operational challenge that doesn't get enough attention in early virtual clinic development planning.
Credentialing Requirements
Every specialist on the platform needs verified board certification, an active medical license in the relevant states, and current malpractice coverage. This isn't a one-time check:
- credentials expire
- licenses renew on different cycles
- malpractice policies lapse
Your physician network needs continuous monitoring, not just onboarding verification.
Case-to-Specialist Matching
Incoming cases need to route to the right reviewer based on subspecialty, case complexity, and provider matching availability. Cleveland Clinic's MyConsult uses Amwell staff to match cases across 3,500 specialists in 550+ subspecialties.
Included Health historically curated what it called the "top 0.1%" of specialists per subspecialty — roughly 1,000 providers. Your matching logic will be simpler at launch, but the data model needs to support increasingly granular routing as your specialist network grows.
Turnaround SLAs
Most platforms commit to a 3–7 day turnaround for a remote second opinion. That commitment needs enforcement mechanisms:
- automated escalation when a case approaches its deadline
- redistribution logic if the assigned specialist is unresponsive
- visibility for ops teams to intervene before an SLA breach
Provider Compensation
Per-case fees, retainers, or revenue share — each model attracts a different type of specialist and creates different incentive structures. This is provider-side economics only; platform pricing is covered in the Monetisation section.
AI's Role in Second Opinion Platforms
AI adds genuine value to an AI second opinion workflow in four places — but none of them replace the specialist.
Case Triage and Routing
Classifying case urgency and matching to the right subspecialist. This is pattern-matching at scale:
- parsing intake data
- flagging high-acuity cases for expedited review
- reducing manual ops overhead
Records Summarization
Extracting key clinical facts from dense medical records so reviewers can orient faster. When a specialist receives a case with hundreds of pages of records, an AI-generated summary that highlights relevant diagnoses, medications, labs, and imaging findings can cut review prep time significantly.
Structured Opinion Generation
AI-drafted opinion templates that specialists review, edit, and sign off on. This accelerates the writing portion of the review without compromising clinical accountability.
Diagnostic Support
Flagging discrepancies between the submitted diagnosis and imaging or pathology findings. This is where AI-assisted pathology has made the most measurable progress.
PathAI's AISight platform (FDA-cleared 2022, expanded 2025) is now deployed at Quest Diagnostics and Labcorp nationwide.
Paige received the first-ever FDA approval for AI in digital pathology and earned Breakthrough Device designation for PanCancer Detect in April 2025. AI-powered pathology algorithms demonstrate roughly 94.6% cancer detection sensitivity, matching senior pathologist performance while processing slides 12–18x faster. The FDA has cleared 38+ AI-assisted digital pathology algorithms as of 2025.
What AI cannot replace: clinical judgment, accountability, and the regulatory sign-off that requires a licensed physician. Teams exploring a HIPAA compliant app builder like Specode AI builder should treat AI as an acceleration layer for specialists, not a substitute.
Monetisation Strategies
There are five proven revenue models for a virtual second opinion platform, and most mature players use more than one.
- Per-case fee (D2C). The most straightforward model. Cleveland Clinic's MyConsult charges $565 per case, $745 with pathology review. Pricing across the market ranges $300–$1,500+ depending on specialty and turnaround. Patients pay directly — simple to implement, but limits volume to patients willing to pay out of pocket.
- Employer/insurer benefit (PEPM). Subscription pricing per employee per month. Grand Rounds historically charged $6–10/employee/month depending on employer size. The value prop is cost avoidance — Accolade/2nd.MD reported employers save roughly $5,000 per consultation, and Cleveland Clinic/Amwell reports health plans save $8,705 per case on average. This is where the largest contract values sit.
- Health system licensing. Annual platform fee for a branded second opinion service — the health system gets the patient relationship and patient records infrastructure, you provide the technology layer.
- Insurance reimbursement. Limited but growing, particularly for oncology where some CPT codes apply. Not yet reliable enough to build a business model around, but worth tracking as a chronic care management app reimbursement pathway expands.
- International. Premium pricing for patients seeking US/EU specialist opinions from lower-income markets. Cleveland Clinic's MyConsult has served patients from 85+ countries — a meaningful revenue line for platforms with strong brand recognition.
Development Approach & Cost
When it comes to how you develop a second opinion platform, there are three paths. The right choice depends on your timeline, budget, and how much of the healthcare app development stack you want to own.
The $400K–$1M+ range for a custom build is realistic once you factor in DICOM viewer integration, multi-role credentialing, EHR connectivity, and patient portal development with full compliance architecture. Industry benchmarks for a basic telehealth MVP (video, scheduling, profiles, payments) start at $40K–$80K in 4–6 months — but a second opinion platform is significantly more complex than a standard telehealth app.
How Specode Can Help
Specode is an AI-powered healthcare app builder — you describe what you want in plain English, and the AI codes it on a HIPAA-compliant foundation. It's not a template system or a drag-and-drop tool. It's a blank canvas where the AI generates your specific application from scratch.
What makes it relevant here: most of the features covered in this guide — patient portals, provider dashboards, role-based access, secure messaging, appointment scheduling, payment processing, custom workflows — are things Specode's AI coder can build from a conversation. You describe the workflow, the AI writes the code. EHR integrations, credentialing logic, case routing — these require configuration and testing against your specific data sources, but the AI handles the initial build.
The compliance layer is built in from day one
- Pro plan includes production hosting with a BAA
- Specode's HIPAA Compliance Agent scans your codebase for violations on demand
- You own 100% of the code — export it, deploy it anywhere, no lock-in
Timeline matters too. A basic telehealth app takes 1–2 weeks on Specode. A more complex second opinion healthcare app with multi-role workflows will take longer, but you're still measuring in weeks, not the 12–18 months of a custom build.
Whether you're building a general diagnostic review platform or a specialized cancer second opinion platform, the starting point is the same: describe what you need, and start building.
Frequently asked questions
It's a platform that connects patients or their providers with specialist reviewers for independent clinical review of a diagnosis or treatment plan. Patients submit medical records, a matched specialist reviews the case (usually asynchronously), and the platform delivers a written opinion — typically within 3–7 days.
A full custom build runs $400K–$1M+ over 12–18 months. White-label solutions start at $50K–$150K with a 3–6 month timeline. AI-powered builders like Specode can get you to MVP in 6–12 weeks at a fraction of the custom cost. The higher end reflects the complexity: DICOM viewer integration, multi-role credentialing, EHR connectivity, and full HIPAA compliance architecture.
Every vendor in the stack that touches PHI needs a signed BAA — cloud infrastructure, messaging, file storage, video, analytics. Beyond that: consent capture for record release, audit logging of every record access, and role-based access controls ensuring each user sees only what they need. Imaging adds another layer — DICOM storage and viewing must also be HIPAA-compliant.
Telehealth apps (Teladoc, MDLive) focus on virtual urgent or primary care — typically live visits for acute issues. Second opinion platforms route complex cases to subspecialists for deep diagnostic review, usually involving medical records, imaging, and pathology. The data surface area, compliance requirements, and specialist workflows are substantially more complex.
Medical imaging requires its own stack. For viewing, OHIF Viewer is the leading open-source, zero-footprint option. For storage, Google Cloud Healthcare API and AWS HealthImaging offer managed DICOMweb-compliant solutions. Self-hosted options like Orthanc and dcm4chee work for teams that need full control. Patient-uploaded DICOM files need to be viewable inline by the reviewing specialist.
Every specialist needs verified board certification, an active medical license in relevant states, and current malpractice coverage. Credentials require continuous monitoring — licenses and policies expire on different cycles. For cross-state cases, the Interstate Medical Licensure Compact (IMLC) covers 41 states but is an expedited pathway, not a single multistate license. California, Florida, and New York are not yet participants.
No. AI accelerates the workflow — case triage, records summarization, structured opinion drafting, diagnostic flagging — but clinical judgment, accountability, and regulatory sign-off require a licensed physician. AI-assisted pathology tools like PathAI and Paige have made real progress (94.6% cancer detection sensitivity, 38+ FDA-cleared algorithms), but they support specialists rather than replace them.
It depends on the approach. A custom build takes 12–18 months. White-label platforms can launch in 3–6 months with limited customization. Specode's AI coder can produce an MVP in 6–12 weeks — a basic telehealth app takes 1–2 weeks on the platform, with multi-role second opinion workflows adding additional build time.