How to Build a Functional Medicine App

Functional medicine has a supply problem hiding in plain sight. IFM has certified just over 2,500 practitioners globally since 2013, while CDC now says three in four American adults live with at least one chronic condition. That is not a market gap. That is a waiting room with no chairs.
Functional medicine app development is how teams start closing that gap without pretending this is just another healthcare app with a better intake form. The build has three quirks you cannot bolt on later:
- Cash-pay billing usually drives the business model, not insurance-first reimbursement.
- Specialty labs like Genova, DUTCH, and GI-MAP often matter more than the LabCorp and Quest flows most EHRs assume.
- Clinical artifacts like the IFM Matrix, ATM framework, and Timeline need to behave like structured product objects, not long notes nobody wants to read twice.
This guide is for healthcare founders, product leads, and engineering teams sizing a real build in 2026. We’ll cover the clinical data model, lab integration patterns, compliance, monetization, build paths, and realistic cost ranges, so you know what to spec, what to negotiate hard, and what to skip.
How do you build a functional medicine app?
Build it around three things generic healthcare software doesn't have: 1) a clinical data model that natively represents the IFM Matrix, ATM framework, and Timeline; 2) specialty lab integration via Fullscript Labs or per-lab HL7 v2 listeners (no major specialty lab ships a public API); and 3) cash-pay billing from day one. Compliance work and lab partnerships dominate the budget; AI compresses everything else.
Key Takeaways:
- Functional medicine apps require a different data model than generic healthcare software. The IFM Matrix, ATM framework, and Timeline are first-class clinical entities. EHR integration is necessary but never sufficient.
- Specialty lab integration is the technical center of the build. No major specialty lab ships a public API. Fullscript Labs (post-Rupa, October 2024) is the shortest path; per-lab HL7 v2 listeners are the long path.
- Cash-pay billing is the default operating assumption, not an edge case. Most FM revenue is cash-pay, specialty tests are routinely classified investigational, and HSA/FSA receipts are the patient-side affordability lever. Build for it on day one.
- The 2025-2026 enforcement risk is at the claims surface, not HIPAA. FDA, FTC, and HHS have stood up an enforcement cadence around DTC pharma, GLP-1 telehealth, and deceptive testimonials. HIPAA infrastructure is table stakes; substantiation files are where the real exposure sits.
- AI compresses scaffolding; it doesn't compress lab partnerships or compliance. UI, intake flows, CRUD, dashboards, and admin panels can shrink 50 to 70% with AI-assisted tooling. Lab integration agreements, BAA negotiations, substantiation files, and clinical accuracy work are the real cost centers.
Why Functional Medicine Software Is a Different Build
Functional medicine software development is not generic healthcare software with a few extra intake questions. Three things change the build from day one:
- too few certified clinicians to serve a massive chronic care population,
- a cash-pay model that makes insurance-first billing tools feel like a fax machine with a login screen,
- clinical workflows like root cause analysis, ATM, and the IFM Matrix that do not fit inside a standard EHR note.
Driver 1: a Clinician Supply Bottleneck
IFM has certified just over 2,500 practitioners globally since 2013, per IFM's 2024 Impact Report, with another 3,100+ AFMCP-trained practitioners listed in IFM's directory across 74 countries. The certified pool is tiny compared with chronic disease prevalence, and it explains why telehealth-first models like Parsley Health and Function Health can scale faster than another beautiful brick-and-mortar clinic.
Driver 2: Cash-Pay as the Operating Model
Most functional medicine work is not insurance-billed. Specialty tests like comprehensive stool analysis and dried urine hormone panels are often classified as “investigational” or “not medically necessary.” So the billing layer has to support:
- memberships,
- bundled programs,
- à la carte consultation fees from day one.
Driver 3: the 15-Minute Visit Does Not Apply
Fee-for-service reimbursement was not designed for 60-to-90-minute consultations. That pushes chronic disease management toward longer intake, async coaching, personalized medicine plans, and care journeys that run for months instead of tidy visit-bound encounters.
Functional Medicine App Market in 2026
There is no clean single number for the US functional medicine app market. The space is usually sized three ways:
- IBISWorld, Alternative Healthcare Providers, NAICS 62139b: $39.0B in 2026, 3.3% five-year CAGR. Closest proxy for provider revenue.
- Grand View Research, US complementary and alternative medicine: $66.69B in 2026, projected 27.8% CAGR through 2033. Includes supplements, yoga, and meditation alongside clinical CAM.
- Verified Market Reports, functional medicine lab testing, North America: roughly $5.5B to $6B in 2026, 8.5% CAGR. Diagnostics slice only.
The honest read: provider revenue grows around 3.3% a year, while broader consumer CAM spending grows 22–28%. That gap is where functional medicine digital health platforms live.
Patient demand brackets the opportunity: 75% of US adults have at least one chronic condition, and 62% reported using some form of CAM in 2024. The bottleneck is clinician supply, not demand. Functional medicine software development sits right in that gap, which makes it a different problem than general-purpose healthcare app development.
Types of Functional Medicine Applications
Functional medicine platform development usually falls into five product categories. A functional medicine application can borrow from several, but one category should still lead. Otherwise, you end up building five half-products instead of one useful system.
Practitioner-Facing FM EHRs
Cerbo, OptiMantra, and Power2Practice. These are clinical-workflow-first systems for healthcare providers running integrative medicine practices. They support specialty labs, supplement dispensaries, structured charting, cash-pay billing, and 60-to-90-minute visits better than a generic EHR designed around insurance-billed encounters.
Intake and Visualization Layers
LivingMatrix is the canonical example. These tools sit next to an EHR rather than replacing it. They focus on IFM-licensed Matrix and Timeline visualizations, MSQ scoring, and structured intake. Practitioners often pair them with Cerbo or another EHR to cover scheduling, billing, and practice management.
Patient-Facing FM Telehealth Platforms
Parsley Health, Wild Health, and Function Health. These are direct-to-consumer or membership-based products, with cash-pay billing built into the model from the start. This is the category closest to general-purpose telehealth app development, but with FM-specific intake, lab panels, and longitudinal care plans baked in.
Lab Aggregator Platforms with Clinical Surface
Fullscript Labs, after the Rupa Health acquisition in October 2024, and Evexia. Practitioners use these as the lab and supplement backbone, usually layered onto a separate EHR. The strength is lab ordering, specialty test access, and dispensary economics. The tradeoff is lighter clinical charting.
Protocol and Health Coaching Apps
Heads Up and coach-led platforms. These focus on care plan delivery, adherence tracking, and async coaching rather than diagnosis or lab ordering. They can overlap with mental health app development and behavioral health app development when the protocol includes stress, sleep, or nervous-system work.
Most production FM apps blend two or three categories. The key decision is which one leads.
What Existing Functional Medicine Platforms Get Wrong
The big gap across the major FM platforms is simple: none of them have turned the IFM Matrix or Timeline into living clinical artifacts inside a full EHR. LivingMatrix has the IFM license, but it is not an EHR. Everyone else gets close with templates, PDFs, or notes. That is the opening for functional medicine app developers in 2026.
Cerbo: Clinical-Grade EHR with No Native Matrix
Cerbo is the closest thing to a clinical-grade FM EHR. It costs $269/mo per prescribing provider and serves 5,000+ practitioners. The platform supports 50+ specialty lab integrations across Genova, Vibrant, DSL, DUTCH, Doctor’s Data, and Mosaic, plus bidirectional Fullscript, strong cash-pay billing, open API access, and webhooks.
Key gaps:
- No native IFM Matrix or Timeline. Chart Parts templates help, but the visual artifact does not ship.
- Charting starts from a blank page, so the learning curve is real.
- No native AI scribe as of early 2026.
OptiMantra: Multi-Modality Strength, FM-Specific Gaps
OptiMantra starts at $99/mo for the first practitioner and $49/mo for each additional practitioner. It fits clinics that run functional medicine alongside acupuncture, naturopathy, chiropractic, or other modalities.
Strengths include a 100,000+ supplement and medication database, native Fullscript and Rupa Labs integrations, recently shipped DeepCura AI scribe, and built-in functional ranges that are tighter than standard reference ranges.
Key gaps:
- Automatic lab integration requires minimum order volume thresholds.
- No IFM Matrix or Timeline tooling.
- Practitioners report form template bugs.
Power2Practice: A4M-Endorsed but Showing Its Age
Power2Practice is the only EMR endorsed by A4M, the American Academy of Anti-Aging Medicine. It was built for functional, integrative, and anti-aging practices, with native Genova and ZRT integrations, Evexia cash-labs integration added in 2025, 30+ IV therapy protocols, and visual progress documentation. Pricing is quote-only and usage-based.
Key gaps:
- Independent reviews show substantial UX complaints.
- E-prescribing is an add-on cost rather than bundled.
- Public information on the AI roadmap is limited.
The honest read: FM-specific design earns loyalty, but workflow speed still draws complaints.
LivingMatrix: The IFM-Licensed Tool That Is Not an EHR
LivingMatrix is the only platform with native IFM-licensed Matrix and Timeline visualizations, built through a direct IFM partnership. It supports PROMIS Global Health outcomes tracking and structured intake-to-Matrix auto-population. Last public pricing was roughly $129/mo plus a $245 setup fee.
Key gaps:
- It is not an EHR, so practices still need scheduling, billing, telehealth, and charting elsewhere.
- Intake forms are not customizable, which is the most-cited limitation.
- No AI features and no specialty lab integrations.
Worth Tracking: Vibrant Practice
This is the AI-native entrant in the FM EHR market, founded by Sunita Mohanty, former Meta AI product lead behind Ray-Ban and Oculus. It has a Hint partnership for membership and DPC infrastructure, claims AI-generated Matrix and Timeline output, and is cash-pay only.
The Functional Medicine Data Model: Why Generic EHRs Don’t Fit
Creating a functional medicine app means modeling clinical data generic EHRs were never built to hold. The IFM Matrix, ATM framework, and Timeline are not note templates. They are core clinical entities. EHR integration with traditional health records systems still matters, but it will not solve the modeling problem by itself.
The IFM Matrix Structure
The Matrix organizes clinical findings into seven biological nodes:
- Assimilation: digestion, absorption, microbiota, respiration
- Defense and Repair: immune system, inflammation, infection
- Energy: energy regulation, mitochondrial function
- Biotransformation and Elimination: detoxification, hepatic and renal clearance
- Transport: cardiovascular and lymphatic
- Communication: endocrine, neurotransmitters, cellular messaging
- Structural Integrity: subcellular membranes, musculoskeletal, organ structure
One naming nuance is worth catching early. IFM’s October 2025 toolkit uses “Mitigation and Clearance” for what other materials still call “Biotransformation and Elimination.” Same node, terminology in transition. In code, use a canonical key like “biotransformation_elimination” and treat “Mitigation and Clearance” as a display alias.
The Matrix center captures Mental, Emotional, and Spiritual state as a first-class entity, not metadata. The bottom band holds five modifiable lifestyle factors: Sleep and Relaxation, Movement, Nutrition and Hydration, Stress and Resilience, and Relationships. That is where lifestyle medicine belongs in the model. The Matrix visual is IFM-licensed. The underlying clinical concepts are not.
ATM and the Timeline Together
ATM stands for Antecedents, Triggers, and Mediators. Antecedents are predisposing factors, like genetics, birth history, family history, or prior medications. Triggers are activating events, like infection, injury, surgery, major stress, or antibiotics. Mediators are ongoing factors that sustain dysfunction, such as chronic stress, mold exposure, dysbiosis, poor sleep, or inflammation.
The Timeline gives those events temporal context across life stages, from prenatal history to the present. The key product insight: TimelineEvent and MatrixCell often describe the same clinical fact from different views. A better 2026 build models them as connected records, not separate forms that make clinicians enter the same fact twice.
GOTOIT as a Workflow State Machine
GOTOIT stands for Gather, Organize, Tell, Order, Initiate, Track. It is the IFM workflow for turning intake, labs, symptoms, and history into a care plan.
For builders, GOTOIT is not just a checklist. It is a patient-case state machine:
- Gather: intake forms, history, and prior records arrive.
- Organize: ATM tags are applied, and lab results map into Matrix cells.
- Tell: the care narrative becomes visible to the clinician and patient.
- Order: interventions are prioritized.
- Initiate: the protocol starts.
- Track: outcomes are measured against MSQ, PROMIS, symptoms, and lab changes.
That framing shows what changes in the record at each step and makes the app easier to build, test, and explain to clinicians.
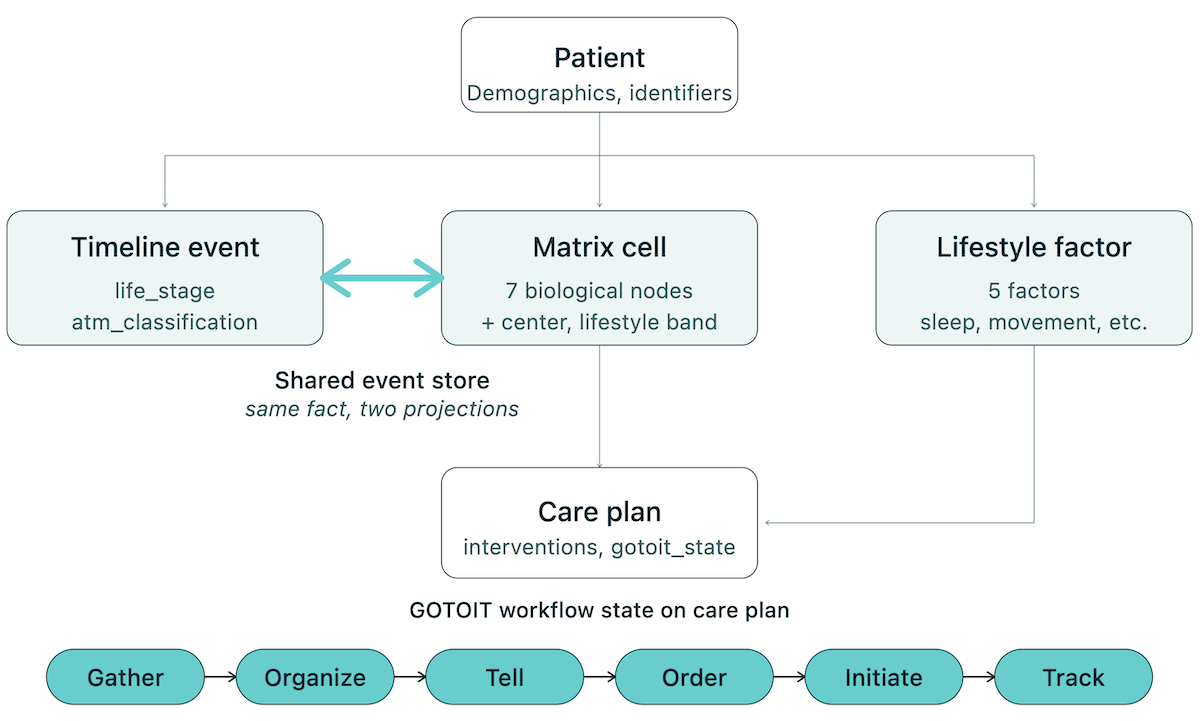
On the implementation side, the schema should keep Patient, TimelineEvent, MatrixCell, LifestyleFactor, LabResult, CarePlan, and GOTOIT state connected rather than scattered across separate forms. That lets one clinical fact appear in multiple useful views: timeline, Matrix, care plan, and progress tracking.
On the IFM IP boundary: model the clinical concept, not IFM’s specific visual layout or copy. LivingMatrix is the only third party licensed to render the Matrix and Timeline visually. The underlying clinical concepts, including the seven systems, ATM, and Timeline life-stage structure, are not copyrighted. You can build your own visualization around the same ideas without copying protected IFM materials.
Must-Have Features of a Functional Medicine App
Functional medicine app features fall into six categories. Together, they separate a real FM product from a generic telehealth app with a longer intake form.
Comprehensive Intake and MSQ
FM intake can run 200 to 400 questions across symptoms, lifestyle, history, and exposures. The IFM Medical Symptoms Questionnaire, or MSQ, should be re-administered every 30 to 90 days. Build for structured question banks, conditional logic, scored sub-domains, and longitudinal tracking.
Matrix and Timeline Visualization
The IFM Matrix and Timeline should auto-populate from intake, support bidirectional editing, and link each Matrix cell to supporting evidence. The Matrix is a clinical reasoning tool, not a static chart. Model the concept, then build your own visual.
Supplement Protocol Management
Supplement recommendations are core infrastructure in FM. Fullscript-grade dispensary integration is the default after Wellevate closed in October 2023. Support products from Designs for Health, Thorne, and Pure Encapsulations, with dosing, timing, duration, adherence, and protocol rotation logic.
Specialty Lab Result Aggregation and Functional Ranges
Functional ranges are standard in FM and mostly absent from generic EHRs. The app needs longitudinal lab tracking, OptiMantra-style dashboard pinning, multi-lab normalization across Genova, DUTCH, and GI-MAP, and PDF rendering when structured lab data is unavailable.
Care Plan and Health Coaching Workflows
Health coaching is a core delivery surface. The app needs group programs, cohort cadence, shared resources, async messaging, coach-to-clinician handoffs, and care plan templates that link each intervention back to a Matrix cell or lifestyle factor.
Patient Engagement and Adherence
Patient engagement in FM is built around a 6-to-18-month protocol. Key surfaces include food logs for nutrition tracking, MSQ-style symptom tracking, wearable overlays for sleep, HRV, and glucose, plus habit streaks for sleep, fasting, and movement targets. Adherence should roll up to the care plan.
Integrating Specialty Labs and Wearables
Specialty lab integration is where functional medicine mobile app development gets real. None of the major labs, including Genova, DUTCH, GI-MAP, Doctor’s Data, ZRT, and Vibrant Wellness, offer public developer APIs. In 2026, the practical choices are HL7 v2 ORU messages, aggregator access, or PDF ingestion. Not FHIR. Not a clean Stripe-style API. Healthcare likes to keep builders humble.
The Major Specialty Labs and Their Integration Modes
The table tells you the real product question. Do you want to support direct lab ordering, structured lab results, PDF storage, or clinical interpretation across gut health, hormone health, and broader biomarker tracking? Those are different builds. A vendor saying “we integrate with Lab X” is not enough. Ask whether it is bidirectional ordering and results, results-only HL7, portal upload, or PDF parsing.
Three Paths to Lab Integration
- Fullscript Labs API. The fastest credible path to broad specialty lab access after Rupa Health’s absorption on October 10, 2024. You get OAuth, sandbox and production environments, and either an Embed library or full REST API. This is usually the cleanest way to support many labs without negotiating every relationship one by one.
- Per-lab HL7 v2 ORU listeners. This is the enterprise route. It means BAAs, partner agreements, message mapping, testing, and months of work per lab. Also clarify the magic phrase: “bidirectional HL7” means orders and results; “results-only HL7” means ordering still happens in the lab portal.
- PDF parsing as a product surface. This is not a temporary workaround. Many specialty lab reports still arrive as PDFs, so the app needs OCR, structured extraction, file storage, and clinician review. Treat PDF ingestion as a first-class workflow or it will become the thing your support team hates forever.
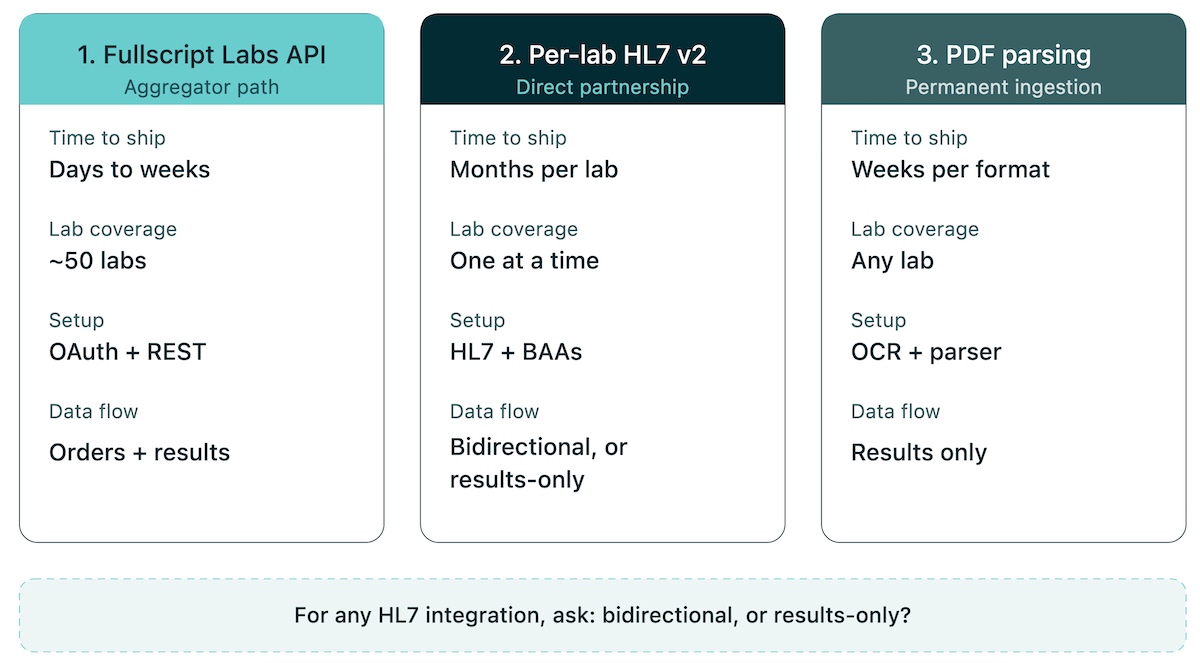
Three integration paths, one binary HL7 question. Path 2 is where AI-assisted builds earn their keep — compressing weeks of HL7 message-mapping and listener work, though BAAs and lab partnerships still set the floor.
Wearable and CGM Integration
Wearable integration in FM is not about celebrating step counts. The useful layer is continuous physiologic data:
- sleep
- HRV
- recovery
- glucose
- activity
- symptom correlation
Most apps should start with Apple HealthKit and Google Health Connect as aggregation layers, then add direct device integrations only where the care model justifies it.
CGM data matters when the protocol targets metabolic flexibility or post-prandial glucose response. The clinical use case is biomarker tracking and remote patient monitoring tied to the care plan, not another dashboard that politely tells patients they slept badly.
The same patterns show up in adjacent telehealth app development work, but FM leans harder on longitudinal data than urgent-care telehealth.
Compliance Reality for Functional Medicine Apps in 2026
Compliance for functional medicine apps is not about proving that FM itself is risky. It is about proving that your product, marketing, vendors, and data flows are not sloppy. HIPAA compliant infrastructure is table stakes. The active risk in 2026 sits closer to claims, testimonials, supplement language, GLP-1 surfaces, and vendor-chain data security.
Marketing Claims Are the Real Enforcement Surface
FM-adjacent telehealth products often drift into risky language before the engineering team notices. Weight-loss programs imply equivalence to branded GLP-1s. Supplement flows make disease-treatment claims. Testimonials quietly skip material-connection disclosures. Review widgets blur the line between real patient feedback and marketing decoration.
That is where enforcement has been moving. The lesson for builders is practical:
- keep substantiation files for every program, supplement, and outcome claim
- make total pricing clear before checkout
- disclose incentives around testimonials
- avoid “equivalent to Wegovy” or “reverses autoimmune disease” style copy unless legal has approved it and the evidence supports it
Annoying? Yes. Cheaper than a regulatory bonfire? Also yes.
Wellness vs SaMD Needs a Product Decision
A wellness app helps users track habits, symptoms, nutrition, sleep, stress, and progress. A Software as a Medical Device product diagnoses, treats, mitigates, or prevents disease. Functional medicine apps can cross that line through copy as easily as through code.
So make the product position explicit. Are you supporting wellness and coaching, or are you making clinical recommendations tied to disease treatment? The answer affects your evidence burden, QA process, documentation, and release controls.
HIPAA, BAAs, and the Vendor Chain
HIPAA does not disappear because the business is cash-pay or “wellness-forward.” If the app handles PHI for a covered entity or business associate, the usual healthcare rules apply.
For FM, the weak spots are often:
- specialty lab portals
- supplement vendors
- payment tools
- AI inference layers
- analytics
- cloud services
Fullscript will sign a BAA, and major AI/cloud vendors may offer BAAs, but you still need to verify current terms before sending PHI anywhere.
That is why data security in FM is a vendor-chain audit, not a checkbox. Map every place PHI flows, confirm every BAA, minimize what each vendor receives, and log access. For the deeper primer, read our guide to HIPAA compliance in healthcare app builds.
Monetization for Cash-Pay Functional Medicine Practices
Most FM revenue is cash-pay. Insurance may cover the conventional edge of a visit, but specialty tests are often classified as investigational. So if you are working out how to develop a functional medicine app that survives past launch, design cash-pay billing first. Appointment scheduling, billing, reminders, receipts, and dunning all inherit that decision.
The five cash-pay models that actually work in FM:
- Membership / subscription: Monthly or annual fee covering visit cadence plus platform access. This is the DPC-style model and usually the cleanest recurring-revenue path.
- Package pricing: Intake, follow-ups, and lab review bundled at a fixed price. Common for onboarding because patients know the cost before they start.
- À la carte consultations: Cash-pay per visit. Easy to understand, but weak for retention unless paired with a membership layer.
- Group programs: Cohort-based gut, hormone, or metabolic programs. Best clinician leverage because one provider can guide many patients through the same protocol.
- B2B2C through employer wellness or clinic networks: FM packaged as a benefit. Slower sales cycle, but higher LTV when it works.
Three details matter in the build. First, HSA/FSA-ready receipts lower patient friction, so get the documentation right. Second, supplement and lab margins can stack on top of consult revenue, but Fullscript’s dispensary position creates a real dependency you should price into the model. Third, no-show fees actually collect in cash-pay care, so do not leave the policy in a PDF nobody reads. Put it into appointment scheduling and automate the reminder, cancellation, and charge flow.
How to Build a Functional Medicine App in 7 Steps
Here is the practical development process for teams that want to build a functional medicine app in 2026. The order matters. If you pick tools before you understand the workflow, the product will look finished long before it becomes useful.
Step 1: Validate the Practice Model and Workflow
Start with the actual care model. A solo practitioner, multi-provider clinic, and SaaS platform for many practices need different schemas, permissions, billing rules, and reporting. Interview at least one practicing FM clinician and watch the workflow end to end before touching code.
Step 2: Define the Data Model
Map the IFM Matrix nodes, ATM, Timeline, and GOTOIT workflow first. Model the clinical concept without copying IFM’s visual IP. Use the schema sketch from Section 4 as the starting point, with TimelineEvent and MatrixCell as connected views over one event store.
Step 3: Choose Your Build Path
Pick the build path before asking for cost. Greenfield development can run $200K to $1M+ over 9 to 18 months. Cerbo or OptiMantra configuration is faster, but limited by their primitives. AI-assisted build with Specode can compress UI, intake, and workflow scaffolding.
Step 4: Wire Up Labs, Supplements, and Wearables
Start with Fullscript Labs API for broad lab access and Fullscript Embed for dispensary workflows. Add per-lab HL7 only when a specific lab is central to the clinical model. Treat PDF parsing as a permanent ingestion path, because many specialty lab reports still arrive that way.
Step 5: Design for Cash-Pay Billing from Day One
Build around memberships, package pricing, HSA/FSA receipts, no-show fees, and automated dunning. Stripe can work with a healthcare-friendly setup, but verify BAA needs across payment, tax, and receipt tools. Do not build insurance billing first and staple cash-pay logic on later.
Step 6: Build the Compliance Posture
Create substantiation files for every product, program, and outcome claim. Add testimonial disclosures, DSHEA-correct supplement label rendering, and a clean BAA chain across labs, dispensary, cloud, and AI vendors. Decide whether the product is wellness or SaMD before marketing decides for you.
Step 7: Pilot With a Real FM Practitioner
Do not launch to “the market” first. Launch to one real clinician and iterate against the GOTOIT workflow until the app fits the practice. The goal is not to impress in a demo. The goal is to disappear into the daily clinical routine.
Tech Stack for Functional Medicine Apps
When deciding how to make a functional medicine app, the functional medicine technology stack should be boring in the right places and opinionated where the workflow demands it. In 2026, experienced healthcare engineering teams usually reach for these defaults:
- Mobile: React Native. One codebase, mature ecosystem, and stronger compliance tooling than most alternatives. Flutter can work, but React Native is the safer default.
- Web: Next.js. Useful for clinician portals, admin tools, and workflows where patient data needs to stay fresh.
- Backend: Postgres for clinical data because Matrix, Timeline, labs, and care plans need relational integrity. Add Medplum or HAPI FHIR when traditional health system interoperability matters.
- HL7 ORU listeners: Mirth Connect or Medplum’s HL7 module. Do not write the parser yourself unless you enjoy debugging sadness.
- Lab integration: Fullscript Labs SDK for the aggregator path. Use direct HL7 only when a lab is central to your clinical model.
- Dispensary: Fullscript Embed for speed. Move to the REST API when you need deeper UX control.
- AI layer: LLM-assisted intake summaries, MSQ scoring, and Matrix narrative generation. Anthropic and OpenAI offer BAAs, but verify current terms.
- Auth and observability: Auth0 or Clerk on BAA-eligible tiers. Datadog or Sentry with PHI redaction.
- Hosting: AWS, GCP, and Cloudflare all sign BAAs. Choose based on team familiarity, not “HIPAA-ness.”
Functional Medicine App Development Cost: Traditional vs AI-Assisted
Functional medicine app development cost depends more on what you skip than on what you build. Lab integration negotiations and compliance work dominate the budget; AI-assisted software development tools compress the rest.
Tenancy isolation, per-practice billing, white-labeling, analytics
For a broader frame on ranges across the wider healthcare space, this healthcare app development guide covers the general-purpose case.
What AI Services Compress
UI scaffolding, form builder logic, intake conditional flows, basic CRUD, admin panels, and dashboard layouts. In the right hands, compression runs 50 to 70%.
What AI Doesn't Compress
Lab integration agreements (lawyer time, BAA negotiations, message mapping), compliance work (substantiation files, audits, DSHEA review), and clinical accuracy (validating MSQ scoring, lab range logic, supplement interaction checks). These are the real cost centers. Pick the build path before pricing.
How Specode Can Help
Specode is an AI healthcare app builder where you describe what you want in plain English and the AI builds it on a HIPAA-ready foundation. For FM teams, that means the parts of the build that don't require deep clinical or compliance work get compressed dramatically:
- Custom data models built to your spec: Entities, fields, relationships, and permissions defined through AI chat. Matrix nodes, Timeline events, ATM tags, MSQ scores, and custom care plans all live as first-class data, not freeform notes.
- AI-built workflows on top: Long-form intake forms, conditional logic, scheduling, provider portals, patient dashboards, and automations get scaffolded from prompts.
- Healthcare integrations by AI: Stripe for payments, EHR/EMR connections (Epic, Cerner), and custom integrations via webhooks for the labs and supplement APIs your protocol depends on.
- HIPAA-ready foundation: Backend hosting BAA included on the Pro plan. Auth, encryption, protected data storage, and audit-friendly workflows built into the deployment path.
- HIPAA Compliance Agent: A built-in multi-agent scanner that audits your codebase for HIPAA violations, categorizes issues by severity, and tracks them over time.
- Full code ownership, no company lock-in: Export the full source any time and deploy anywhere. No platform lock-in.
The result is a team-of-two-or-three operating model:
- A domain expert (often a practicing FM clinician) who owns the workflow.
- An AI-assisted builder (Specode) that compresses scaffolding, CRUD, and integration glue.
- A healthcare engineer or compliance reviewer for the parts that don't compress: specialty lab partnerships, claim substantiation files, clinical edge cases.
If you're working out how to create a functional medicine app, book a Specode demo and we'll walk through the build path that fits your practice model.
Frequently asked questions
Software that supports root-cause clinical workflows: long-form intake, the IFM Matrix and Timeline, specialty lab aggregation, supplement protocol management, and cash-pay billing. It replaces or layers onto a generic EHR.
HIPAA at the standard level plus FTC substantiation rules, DSHEA for supplement label claims, FDA scrutiny if the app crosses into SaMD territory, and state-by-state telehealth licensure.
AI compresses intake summarization, MSQ scoring, Matrix narrative generation, lab interpretation drafts, and care plan templating. It does not replace clinical judgment or compliance work.
FHIR for traditional EHRs, HL7 v2 ORU for specialty labs (no major specialty lab ships a public API), and aggregators like Fullscript Labs and Evexia for fast multi-lab coverage.
The IFM Matrix, the ATM framework, and the Timeline are first-class clinical entities, not freeform notes. Standard EHR schemas don't represent biological-system nodes or temporal antecedent-trigger-mediator relationships natively.
4 to 6 months for a solo-practitioner MVP, 8 to 12 months for a multi-practitioner clinic platform, and 12 to 18 months for a multi-tenant SaaS.