How to Launch a Telehealth App in 60 Days Without Building Everything From Scratch

You've scoped a telehealth product, lined up the clinical side, and now a build estimate lands that says nine months. Most of those months go to rebuilding plumbing that already exists: auth, hosting, video, e-prescribing, payments. Then there's the opposite reflex, where "ship fast" gets read as "ship a throwaway prototype" that can never touch real patient data.
How to launch a telehealth app without either mistake comes down to a reframe. 60 days to a live, HIPAA-ready MVP is realistic when you make the vendor calls early and stop hand-building commodity infrastructure. A from-scratch custom build runs 4 to 9 months. The 60-day version gets there because the compliant foundation comes with the platform, already wired, instead of assembled from parts after the fact.
The sequence and the vendor decisions set your timeline. The feature checklist matters less than founders expect. The market gives you room to get it right: US telehealth sits around $65.35B in 2026, and adoption has settled into a steady 14 to 17% of outpatient visits, so you're building into something real without overselling it. Curology and Hims already proved the D2C model works. Your job is to launch a telehealth business in 2026 without losing two quarters to infrastructure.
How do you launch a telehealth app in 60 days without building it all from scratch?
Make the three vendor decisions early (async versus synchronous, your e-prescribe and pharmacy-fulfillment integrations, and which vendors sign BAAs), then build only your clinical workflow and data model on top of prebuilt, HIPAA-ready infrastructure. A from-scratch custom build runs 4 to 9 months; the 60-day version works because the compliant foundation and backend hosting BAA already ship with the platform.
Key Takeaways:
- 60 days holds when you make the vendor decisions in week one. A live, HIPAA-ready MVP is realistic when you stop rebuilding commodity infrastructure and lean on a compliant foundation that already exists. A from-scratch custom build runs 4 to 9 months.
- An async-first MVP needs only four components. Structured intake, asynchronous clinical review with secure messaging, e-prescribing plus pharmacy fulfillment, and payments. Going async-first removes the real-time video layer and live scheduling that make a synchronous build heavy.
- Three vendor decisions gate your timeline. Async versus synchronous, your pharmacy and e-prescribe integrations (verify documented API access before scoping), and which vendors sign BAAs. Treat every PHI-touching BAA as baseline, and anchor compliance to the existing Security Rule and current OCR enforcement, since the 2026 update is still proposed.
- Build only what differentiates you, and plan the data model now. Buy the commodity layer (auth, hosting, video, e-prescribe, payments) and spend your engineering time on your clinical workflow and patient experience. Capture structured intake and images from day one so you can add an AI layer later without re-architecting.
What your telehealth MVP actually needs
Ask a founder what their telehealth MVP needs and you'll get a feature list: live video, a scheduling system, EHR integration, native iOS and Android apps. Most of that is deferrable, and going async-first lets you skip the heaviest parts entirely.
A D2C async telehealth MVP needs four things:
Structured patient intake and onboarding
A store-and-forward questionnaire that captures medical history and symptoms, plus photos where the condition calls for them.
Asynchronous clinical review plus secure messaging
A provider reviews the submission on their own schedule and messages the patient back. No live visit.
E-prescribing plus pharmacy fulfillment
Getting the prescription written and getting it filled, which are two separate integrations (more on that in the next section).
Payments
Cash-pay checkout through Stripe is enough for a D2C launch.
Async-first is what keeps the list at four instead of forty. Store-and-forward removes the real-time video layer and the live-visit scheduling that eat most of a synchronous build, and for conditions like dermatology it's the right clinical model anyway.
Auth and role permissions, plus the HIPAA-compliant infrastructure underneath, sit below all four as table stakes. They come with the platform. You don't spend weeks building them, and they won't win you a patient.
The four are easy to name. The vendor decisions behind intake-to-fulfillment are what actually gate your timeline.
The three vendor decisions that gate your timeline
Most launch delays trace back to telehealth vendor selection: calls made late, or made wrong, and discovered in week six. Three of them cause most of the damage.
Async or synchronous: which should you build?
Choose async-first wherever the condition allows it.
This is a build-scope decision as much as a clinical one. Async store-and-forward means a patient submits intake and photos, and a provider reviews on their own schedule. No calendar coordination. That removes the real-time video layer and the live-visit scheduling, which is where a synchronous build spends most of its effort. For dermatology-type conditions that read well from a questionnaire and images, async is the right clinical model anyway. An async telehealth platform is less to build.
Sync earns its place when real-time assessment is clinically necessary. Make the call on purpose, rather than defaulting to video because every demo has it.
Pharmacy: do you e-prescribe, fulfill, or both?
Verify documented API access before you scope a single hour of development.
Founders collapse two different integrations into one word. E-prescribing transmits the prescription to a pharmacy over the Surescripts network. Fulfillment is a mail-order pharmacy that fills the script and ships it. Separate vendors, separate builds.
For e-prescribing, use certified middleware. DoseSpot is Surescripts-, Drummond-, and ONC-certified and built for telehealth workflows, either as an embedded UI you drop straight in (its JumpStart product, 70+ API calls) or a full-API native integration, and it handles those certifications for you.
The integration path sets your timeline:
- Embedded middleware: weeks
- A full custom API: months
- Self-certifying with Surescripts directly: 12 to 18 months and $500k-plus
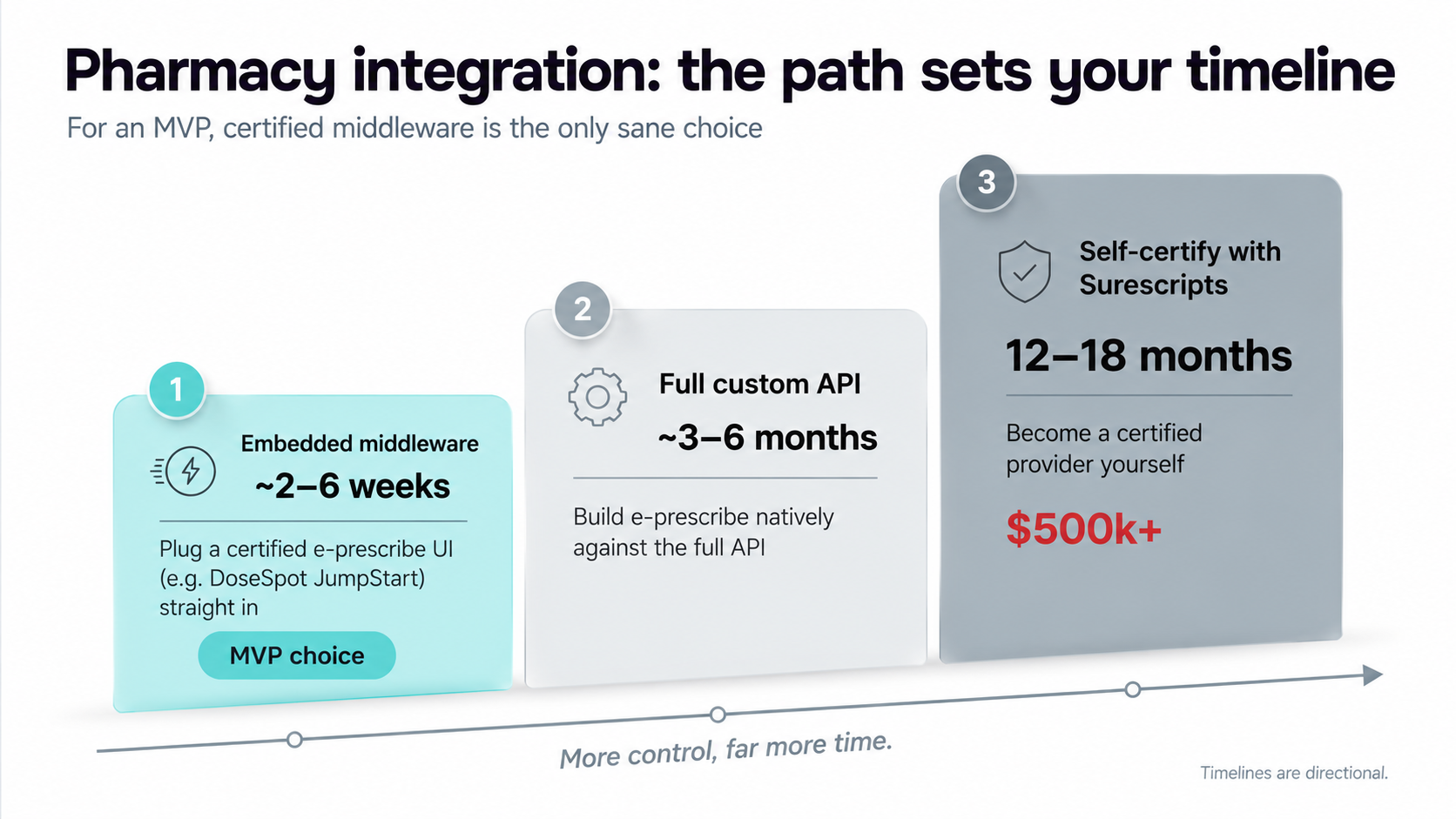
For an MVP, the middleware is the only sane line on that list.
For fulfillment, treat it as a category rather than a fixed name. The canonical D2C option consolidated when Truepill was acquired by LetsGetChecked in 2024 and restructured, so confirm any partner is live and shipping against a documented API before you commit. And if you'll prescribe controlled substances, EPCS adds prescriber identity proofing plus two-factor auth, with onboarding that can run about 2 weeks. Start it early.
HIPAA infrastructure: who signs a BAA?
Every vendor that touches PHI signs one.
Video, messaging, hosting, email, pharmacy, EHR: if a service handles patient data, it needs a BAA. That's baseline. Sign them as you stand up the rest of your HIPAA compliant telehealth stack, the way you configure auth, so they never become a pre-launch scramble. We mapped the full vendor-chain version of this in our HIPAA compliant health app guide.
Anchor your compliance to what's actually in force. The HIPAA Security Rule update is still a proposal as of 2026, so build to the existing Security Rule and current OCR enforcement. On prescribing, the DEA's controlled-substance telehealth flexibilities are temporary, extended through Dec 31 2026, with no permanent rule yet.
One shortcut here is real: a platform that includes the backend hosting BAA in its license takes one of these negotiations off your plate entirely. This is exactly the gap a branded telehealth platform is built to close, since the BAA and the compliant hosting layer ship as part of the same license.
Make these three calls in the first couple of weeks and the 60-day timeline holds. Push them to week six and it turns into a rebuild.
How to launch a telehealth app in 60 days, day by day
A 60-day telehealth launch runs as three 20-day phases, each one gated by a decision or a deliverable. Sequence the gating work first and the date holds; treat the 60 days as a countdown and it slips. The phases barely overlap, but every decision in the first one quietly sets up the next two.
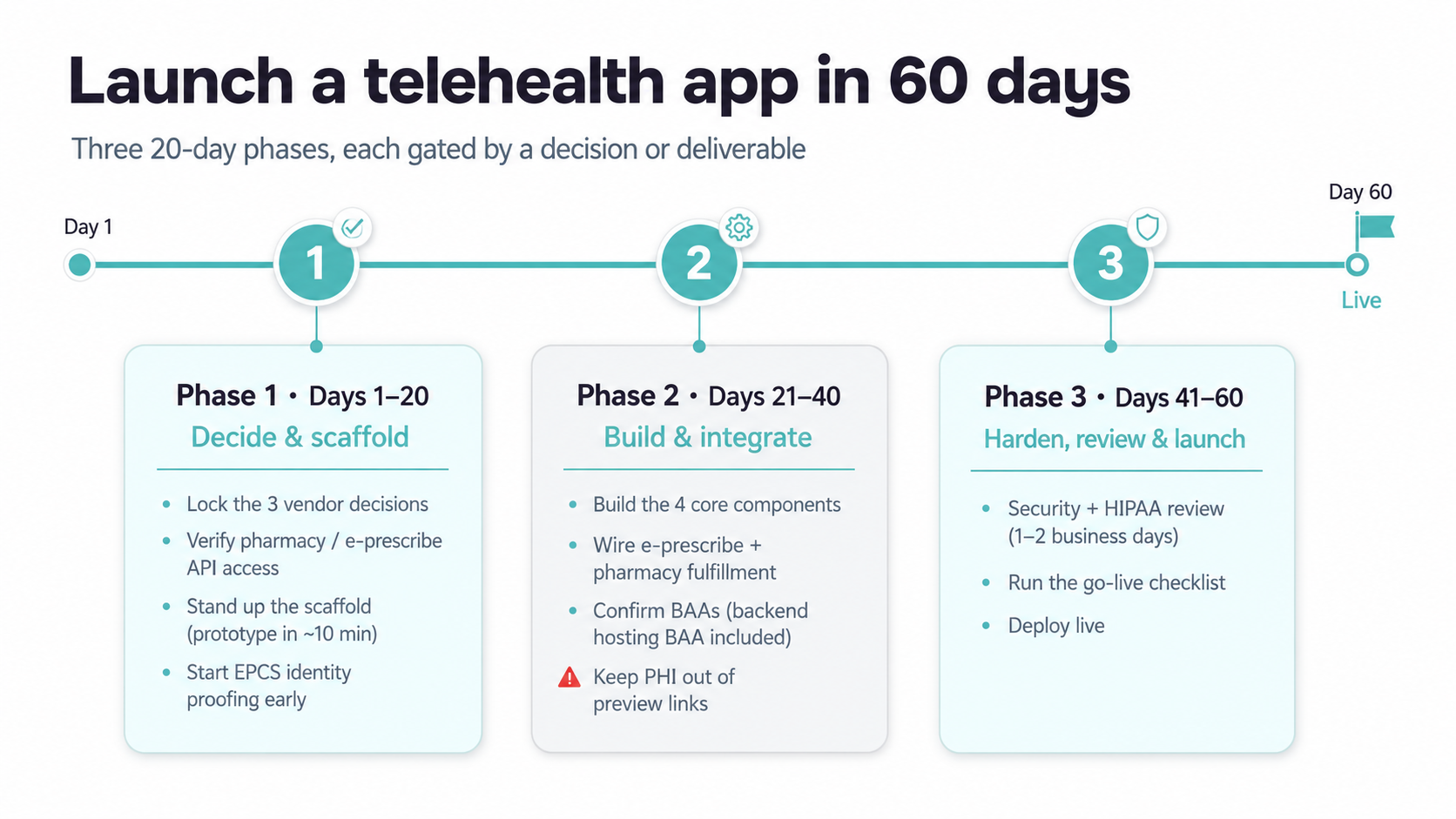
Days 1-20: decide and scaffold
The first 20 days are mostly decisions, with very little code. That's the point.
- Lock the three vendor decisions from the last section. None of them should still be open on Day 20.
- Verify pharmacy and e-prescribe API access, and choose your integration path. A partner with no usable API is the classic timeline-killer, so this is the gate for the whole phase.
- Stand up the scaffold. A working prototype takes about 10 minutes, and a basic production-ready build runs 10 to 14 days on prebuilt HIPAA components, where the compliant hosting and security layer comes already wired. That's what makes the 60-day math work.
- If you're prescribing controlled substances, start EPCS identity proofing and two-factor auth now. Onboarding a prescriber can take about 2 weeks and runs in parallel, so it can't wait until the day you need it.
Days 21-40: build and integrate
Now you build, against decisions that are already made.
- Build the four components against the locked decisions: structured intake, async review with secure messaging, e-prescribe with fulfillment, and cash-pay checkout.
- Wire the e-prescribe and fulfillment integrations you verified in phase one. Async-first pays off here, with no real-time video layer to build or harden.
- Confirm the BAAs. The backend hosting BAA is included on Specode Pro; third-party vendors you added, like CometChat for video, sign their own. That's one negotiation already off the table, which is part of why this phase fits in 20 days.
Hold one discipline the entire time: keep real PHI out of preview and demo links. Those URLs aren't HIPAA-covered, and a shared preview running live patient data is the kind of thing that becomes an OCR conversation later.
Days 41-60: harden, review, launch
Two gates stand between you and live.
- Run the pre-go-live security and HIPAA review. On Specode that's a 1 to 2 business-day check of the codebase before you're cleared to handle real patient data.
- Clear the go-live checklist, then deploy:
- GitHub repo with the Specode team added
- Vercel for the frontend
- Mailgun on its HIPAA-compliant email plan
- custom domain DNS pointed and verified
- every PHI-touching BAA signed
The 60 days held because the expensive decisions got made while they were still cheap to change. Leave them open and no amount of fast building buys the time back.
What to build custom
The instinct is to build all of it yourself, to "own" the product end to end. Most of the stack doesn't reward that.
Buy the commodity layer: auth, hosting, video, e-prescribe, payments. These are the vendor decisions you already locked in week one. The infrastructure is solved and cheap relative to your engineering time, and rebuilding any of it burns weeks while leaving your app no better than the one that just bought it.
Build the parts that are actually yours: your clinical workflow and protocol logic, your data model, your patient experience, and the AI or triage layer when you add it later. That's where a D2C telehealth product earns its place, and it's the only code worth your engineers' attention.
You own 100% of your code and can export it anytime, so leaning on commodity infrastructure costs you nothing in independence. We go deeper on the split in our D2C telehealth launch guide.
Drag-and-drop speed with someone else's product underneath it is a trade-off, and it's not the only one available: a white label telemedicine platform gets you the branded front door and the fast launch while leaving the code and the workflows yours.
The AI layer: plan for it now, build it later
Founders make one of two mistakes with AI: they over-build it into v1, or they design as if it'll never arrive. Most D2C telehealth apps don't need it there. What matters now is the data you capture, since that's what any AI layer works with later.
Build it later. AI dermatology and image-analysis APIs are a mature white-label category now: Autoderm, Skinive, PerfectCorp. They produce structured triage output and deliberately stop short of diagnosis, the regulatory boundary you design around, and they drop in later as REST integrations.
Plan for it now. Capture structured intake and images from day one. Condition-adaptive intake, the kind that adapts its questions to what the patient reports, is what makes a later AI layer useful; generic forms throw away the signal a model would need.
One caution. A 2021 UK teledermatology app shared patient imaging without sufficient consent, a high-profile breach. Plan the data and consent layer with the same BAA discipline from the vendor-decisions section.
Own your data model and keep the compliant infrastructure handled, and the AI layer is something you switch on later. Get the foundation right in telehealth app development and you build the compliant base in days, then add the intelligence when the data's ready.
That's the foundation we built Specode to give you: compliant from day one, yours to export. If it's useful to see what that looks like first, you can book a demo.
Frequently asked questions
Three 20-day phases: decide and scaffold, build and integrate, then harden and launch. Each one is gated by a vendor decision or a deliverable rather than a guess.
Three: async versus synchronous, your pharmacy and e-prescribe integrations (verify documented API access first), and which vendors sign BAAs. Make all three early or the timeline slips.
Every vendor that touches PHI signs one before you handle real patient data. That's baseline, and a platform with the backend hosting BAA included removes one of those negotiations.
Async (store-and-forward) is faster. It skips the real-time video layer and live scheduling, and fits conditions that read well from a questionnaire and photos, like dermatology.
Under DEA temporary flexibilities extended through Dec 31 2026, you can prescribe Schedule II through V via audio-video with no prior in-person visit. Plan EPCS onboarding early; no permanent rule exists yet.





